2852
4D flow MR measurements for functional assessment of idiopathic pulmonary arterial hypertension: comparison between patients and healthy volunteers1Center for Biomedical Imaging Research, Department of Biomedical Engineering, School of Medicine, Tsinghua University, Beijing, People's Republic of China, 2Department of MR, Beijing Shijitan Hospital of Capital Medical University, 3Department of Pulmonary Vascular Disease and Geriatric Medicine, Beijing Shijitan Hospital of Capital Medical University
Synopsis
We applied parameter analysis in 4D flow imaging for pulmonary artery hypertension (PAH) and compare the MR parameters between five patients with iPAH and five healthy volunteers. Compared with healthy volunteers, patients with idiopathic PAH have more retrograde flow in MPA, enlarger area of MPA, higher peak acceleration. And Plane-to-plane variations of these parameters were evaluated using the Bland-Altman comparisons, some parameters have relatively low variations which means they can be calculated through 2D flow imaging. In conclusion, MRI results show that the effect of increased pulmonary artery pressure and resistance has influence the flow in MPA.
Purpose
Assessment of pulmonary artery hypertension is drawing more and more attention from clinicians. Right Heart catheterization (RHC) is the current reference standard for the diagnosis and assessment of PAH, but it is invasive and carry a small risk of severe complications. Other methods such as Doppler ultrasonography [1] and CT [2], while Doppler ultrasonography leads to inaccurate measurement in some cases and CT fails to give some functional parameters. 3D phase-contrast MRI (4D flow MRI) makes it possible to quantify the velocity and flow accurately, so it can be the best noninvasive method to evaluate the PAH [3]. Therefore, goals of our study were to apply parameter analysis in 4D flow imaging for PAH and compare the MR parameters between patients with iPAH and healthy volunteer.Materials and Methods
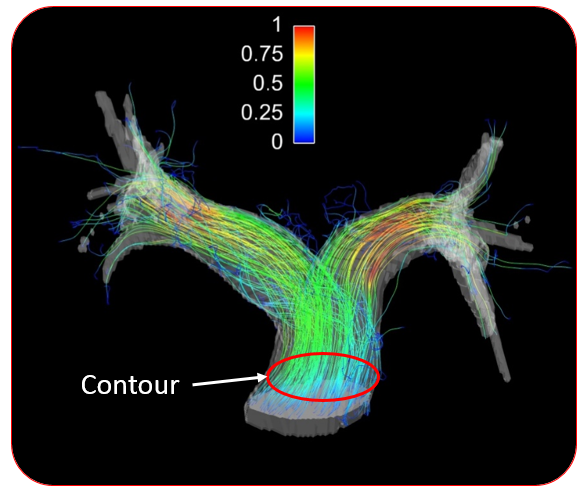
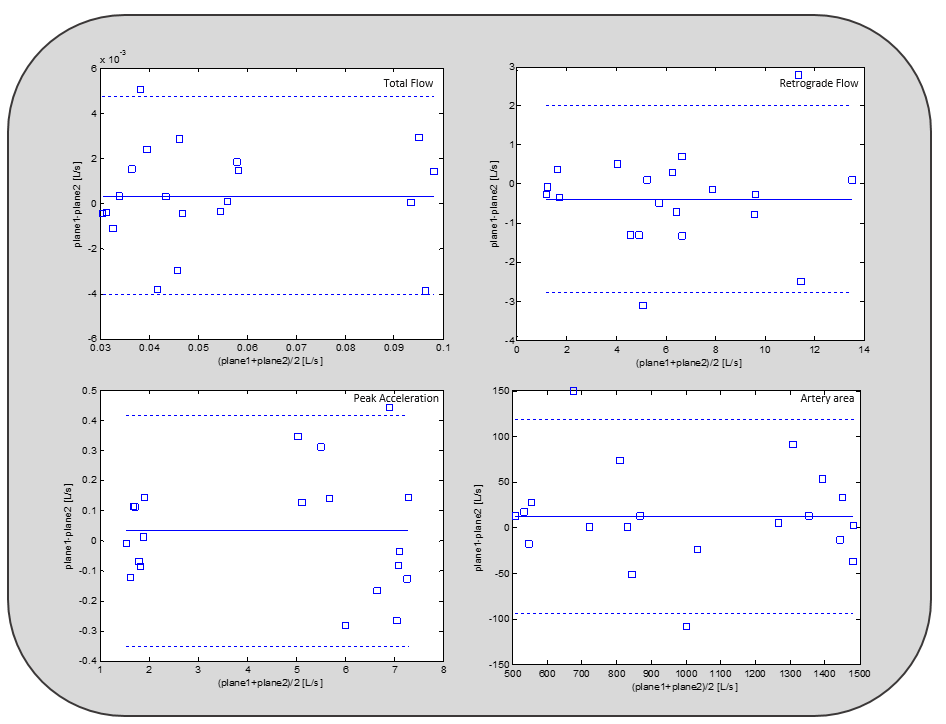
MRI Scan: Five patients with idiopathic PAH (iPAH) (mean age 42 years) and five healthy volunteers were scanned using 4D flow sequence in this study. The experiments were performed on a 3T MRI scanner (Philips Medical Systems, the Netherlands). The MR imaging parameters included: TR/TE = 4.6/2.4ms, Flip Angle = 10 deg, FOV = 200 x 200 mm2, VENC = 150cm/s, Temporal Resolution = 39-45ms. Image Analysis: MPA was segmented from PC-MRA data [4] using Mimics (MIMICS, Materialise Inc., Belgium). 6 2D cross-sections were selected in MPA, and all morphological and functional parameters of analysis planes in MPA (Fig.1) from MR were calculated using Matlab R2013b (The MathWorks, MA, USA). Statistical Analysis: Plane-to-plane variations were evaluated using the Bland-Altman comparisons between parameters from six planes in each patient. Averaged MR parameters from 6 planes in each case were used for the comparison of MRI parameters between patients and healthy volunteers. P values were calculated through t-test to determine the significance of the differences.Results
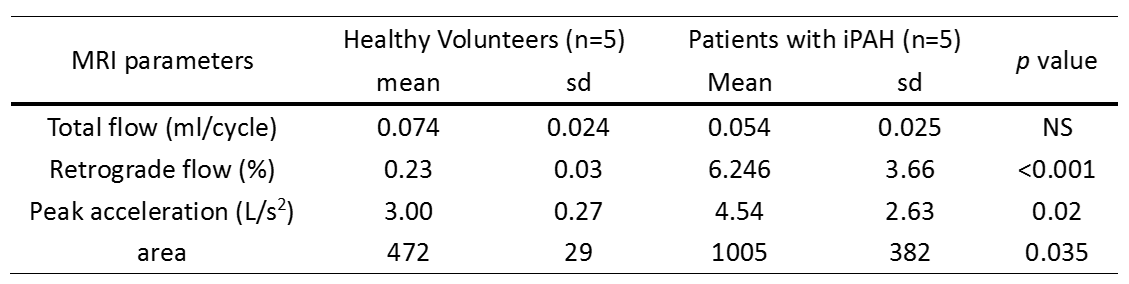
Figure.2 demonstrated plane-to-plane variation of different parameters from MRI, while total flow, peak acceleration had relatively small variations. In comparison with the healthy volunteers (Table.1), patients with iPAH showed a significantly more retrograde flow, which means the retrograde flow in the main pulmonary artery could be a characteristic of PAH. In fact, we observed the vortices in MPA existed in 4 of 5 cases through the visualized streamlines as in Fig 1. The Patients also had enlarged main pulmonary artery compared with healthy volunteers, for patients with iPAH the increase of area of MPA could be the results of compensatory for high pulmonary artery pressure. Patients also had higher peak acceleration and lower total flow (not significant). Other parameters didn’t show any significant difference.Conclusion and Discussion
In this study, MRI results show that the effect of increased pulmonary artery pressure and resistance has influence the flow in MPA. Some parameters (retrograde flow and area of MAP) can be used for diagnose the PAH, other parameters may have overlap between patients and healthy volunteers. What’s more, we verify the plane-to plane similarity of some parameters, so we can get these parameters simply from 2D PC MRI with a much shorter scanning time. But we should realize that this study only included a limited sample size of patients so we should treat the results carefully. Another limitation of this study is the consistency of sample (healthy volunteers have similar ages).Acknowledgements
This work was supported by Capital characteristic project (z141107002514070).References
[1] Fisher M R, Forfia P R, Chamera E, et al. Accuracy of Doppler echocardiography in the hemodynamic assessment of pulmonary hypertension. American journal of respiratory and critical care medicine, 2009, 179(7): 615-621.
[2] Galiè N, Torbicki A, Barst R, et al. Guidelines on diagnosis and treatment of pulmonary arterial hypertension[J]. European heart journal, 2004, 25(24): 2243-2278.
[3] Sanz J, Kuschnir P, Rius T, et al. Pulmonary arterial hypertension: Noninvasive detection with phase-contrast mr imaging 1[J]. Radiology, 2007, 243(1): 70-79.
Figures