2841
Real-time monitoring of Exercise Stress using Spiral Flow MRI1National Heart Lung and Blood Institute, National Institutes of Health, Bethesda, MD, United States
Synopsis
Interventional cardiovascular MR exams can augment catheter procedures with simultaneous functional measurements. This preliminary work implements an accelerated spiral acquisition to measure real-time, beat-to-beat cardiac output changes during exercise stress induced using a MR-compatible ergometer. At rest, the beat-to-beat variation in cardiac output had a coefficient of variation of 19.1 ± 16.8%. Using this high temporal resolution sequence, a significant increase in cardiac output (5.23 L/min to 8.39 L/min) was measured between rest and exercise sustained at 160-180 W.
Introduction
Measurements of cardiac flow and function during exercise stress has potential to be sensitive to early indicators of cardiovascular dysfunction, and real-time measurements of cardiac output have been shown to compliment interventional cardiovascular MR procedures [1-2]. As conventional ECG-triggered, segmented cardiac imaging is not robust under exercise; we investigate the sensitivity of real-time phase-contrast flow MRI to measure cardiac output during exercise on a MRI compatible ergometer. Such measurements can help towards the diagnosis and treatment management for patients with cardiovascular dysfunction.Methods
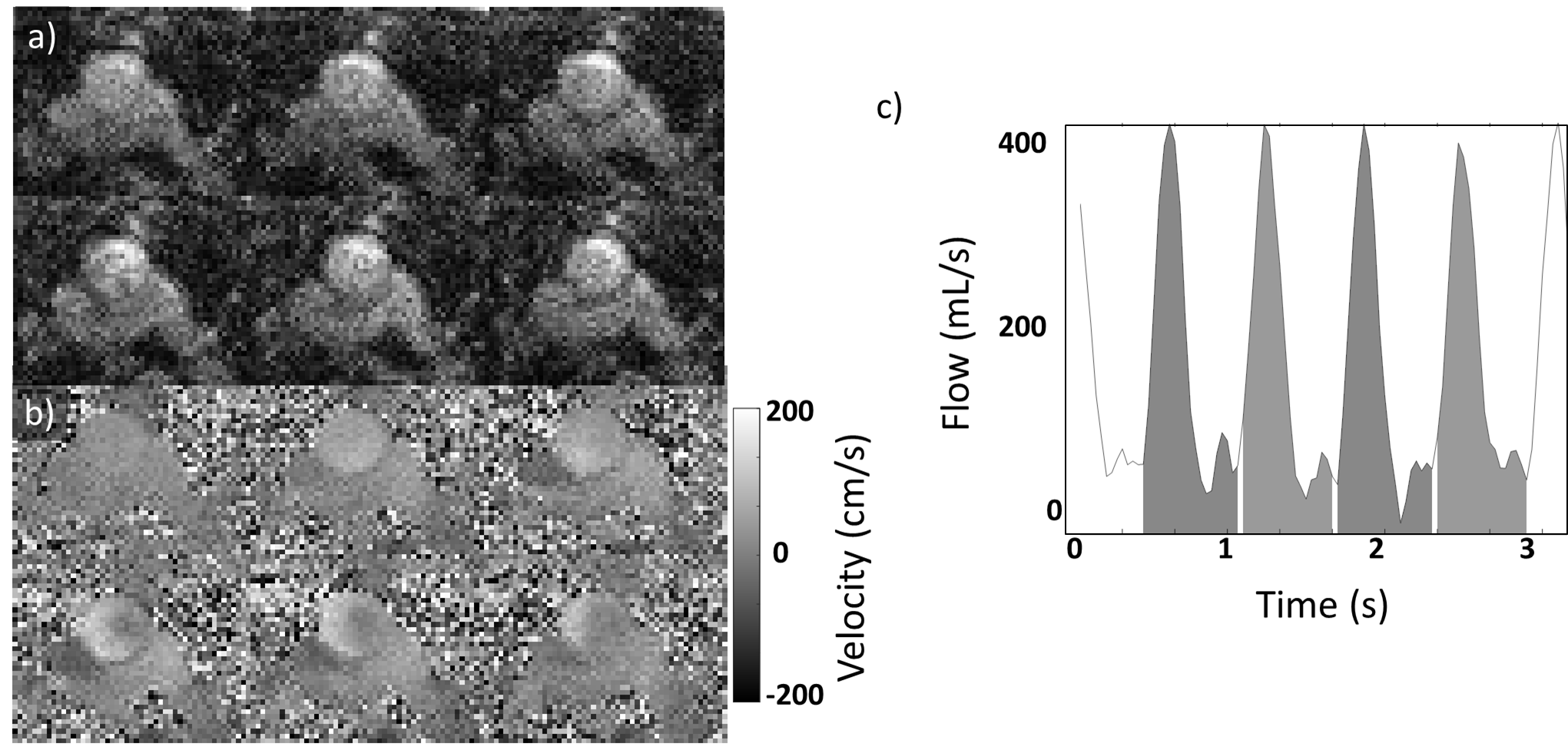
Real-time flow MRI: Scanning was performed on a 1.5T scanner (Aera, Siemens Healthcare, Erlangen, Germany), with phased array coils (Body 18) on the anterior and posterior chest. Imaging slices were planned transverse to the ascending aorta, just superior to the valve. An eight-shot spiral GRE sequence with TE/ TR = 1.6/ 8.9 ms, 128 x 128 matrix, acceleration factor 4 to yield a temporal resolution of 36 ms. A venc of 150 cm/s was applied at rest and 200 cm/s during exercise. Images were reconstructed offline using iterative conjugate gradient SENSE [3-4].
Cartesian Flow MRI: Reference phase-contrast images were acquired in matching orientations with the following parameters at rest: 256 x 256 matrix, TE/TR = 3.6/23.6 ms, 3 averages, acceleration factor 4, venc of 150 cm/s. Data was retrospectively ECG-triggered in to 50 cardiac phases.
Exercise Protocol & Analysis: Human studies were approved by the institutional review board at NHLBI or Children’s National Medical Center. An MRI compatible ergometer (Cardio Step, Ergospect, Innsbruck, Austria) was mounted on the scanner table (figure 1), resistance was controlled via a PC in the control room. Real-time flow measurements were acquired at rest and at two stages of increasing exercise (mild: 100-120W and medium: 160-180W, sustained for five minutes at 60 rpm) in two healthy volunteers. Data was acquired continuously for 3.5s at each intensity level and ROIs were drawn using Siemens Argus analysis software. Beat-to-beat cardiac output was estimated by integrating between cycles of peak flow (figure 2). In addition, three healthy volunteers were scanned at rest for approximately 30s to gauge the variation of estimated beat-to-beat cardiac output.
Results
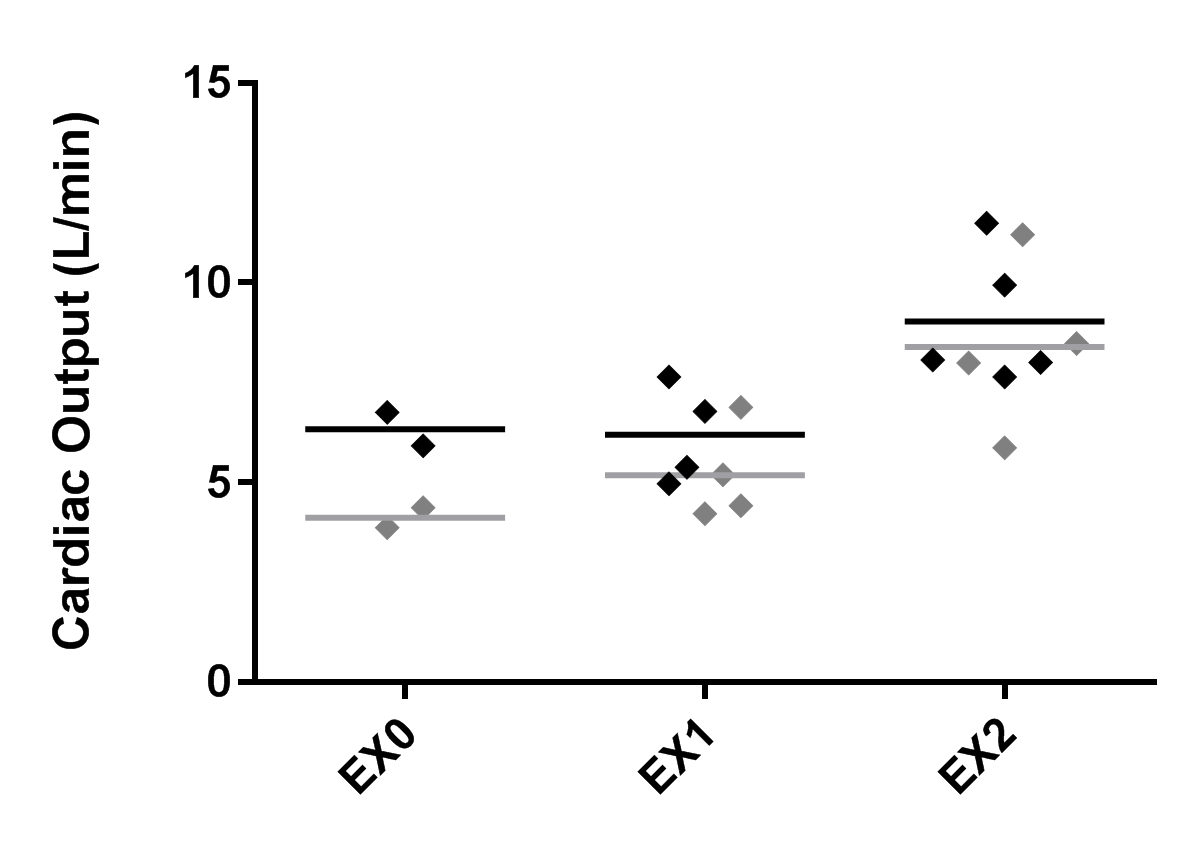
Exercise paradigms were successfully completed without significant shifts to the imaging plane. A significant increase (p < 0.01, ANOVA) between rest (5.23 ± 1.57 L/min, mean ± std), mild intensity (5.69 ± 0.71 L/min), and medium intensity exercise (8.39 ± 0.45 L/min) was detected using the real-time flow imaging (figure 3). From the real-time measurements, the mean heart rate increased from 60.2 ± 0.8 bpm at rest, 82.6 ± 3.7 bpm at mild intensity and 89.3 ± 2.6 bpm at medium intensity. At rest, an average of 19% difference was measured at rest between cardiac output estimated by the ECG-gated Cartesian acquisitions and the mean real-time spiral cardiac output. ECG-dependent sequences did not have a robust triggering during exercise and were not analyzed under this paradigm. During the 30s of continuous scanning, a coefficient of variation of 19.1 ± 16.8% (mean ± std) was measured for the beat-to-beat estimation of cardiac output.Discussion
In this preliminary study, we have implemented a real-time flow sequence with an MRI-compatible ergometer to measure increased cardiac output, though the mild intensity was not sufficient to provoke a significant change in the healthy volunteers. A large variation was measured between healthy volunteers’ cardiac output at rest, which may be due to a limit of the number of heartbeats during a 3.5s acquisition. Variation of cardiac output over the 30s acquisition at rest may be attributed to the influence of respiration, however further investigations are required to understand this and the potential discrepancy with ECG-triggered Cartesian imaging. The real-time method does not rely on gating, thus was more robust than ECG-triggered sequences during the exercise stress, and has the potential to supplement interventional cardiovascular MR exams.Acknowledgements
This work was supported by the NHLBI DIR (Z01-HL006039, Z01-HL005062).References
[1] N. Barber and V. Muthurangu. JCMR, 2016; 18(Suppl 1):P178. [2] E. Ako, et al. JCMR, 2016; 18(Suppl 1):O69. [3] M.S. Hansen, et al. Magn Reson Med., 2013; 69(6):1768-76 [4] K.P. Pruessman, et al. Magn Reson Med., 2001; 46:638–651.Figures