2829
Independent phantom validation of Metric Optimized Gating for fetal cardiovascular phase-contrast flow imaging and application in a second center1Clinical Sciences Lund, Clinical Physiology, Lund University, Skane University Hospital, Lund, Sweden, 2Biomedical Engineering, Faculty of Engineering, Lund University, Lund, Sweden, 3Diagnostic Radiology, Lund University, Skane University Hospital, Lund, Sweden, 4Laboratory of Computing and Medical Informatics, Aristotle University, School of Medicine, Thessaloniki, Greece
Synopsis
Fetal cardiovascular MRI may enhance clinical flow measurements. The lack of fetal ECG for gating however makes phase contrast (PC) flow quantification challenging. Metric Optimized Gating (MOG) overcomes this limitation, but is currently applied only in a single center. We provide independent pulsatile-flow phantom validation of MOG PC-MRI for fetal flow volumes and heart rates, and measurements in human fetuses in a second center. Flow by MOG agrees with timer/beaker and gated flow quantification, and gives pulsatile fetal flow curves in a second center, suggesting MOG PC-MRI as a reliable tool for fetal flow quantification in more centers.
Introduction
Fetal cardiovascular magnetic resonance imaging (MRI) is an emerging tool with the potential to enable physiological measurements currently unavailable by fetal ultrasound. The lack of an ECG signal makes fetal time-resolved flow quantification challenging. Metric Optimized Gating (MOG)1 can potentially overcome this limitation, combining oversampling of each heartbeat with retrospective numerical optimization to find underlying RR-intervals, but currently only used in a single center. If shown reproducible at multiple sites, MOG may contribute further to fetal cardiovascular research and potentially make its way into clinical routine. Therefore, this study aimed to provide independent phantom validation of MOG PC-MRI at flow volumes and heart rates corresponding to the fetal cardiovascular system, and to evaluate MOG PC-MRI in human fetuses at a second center.Methods
The flow phantom consisted of a pulsatile pump and a flow rectifier connected to a water tank, originally designed for pulsatile flow and vortex ring formation experiments2. The flow rectifier nozzle was extended with a plastic tube with 6.3mm inner diameter, comparable to the umbilical vein and fetal descending aorta towards term. The pump was set to 145 bpm and a trigger signal was forwarded to the MR system for image gating. Two sequences for time-resolved 2D PC-MRI were acquired in a transversal plane perpendicular to the tube: 1) The MOG sequence with simulated gating frequency as previously described1 with parameters as below, and 2) a conventional retrospectively gated PC-MRI sequence with matching parameters using the pump trigger signal for gating. Background phase offsets were estimated after stopping the pump, using PC-MRI acquisitions with matching parameters and an averaging factor (NSA) of 50 for improved SNR. Background phase correction was performed by subtraction of a first-order polynomial fit derived from the averaged acquisition. Timer/beaker measurements were used as flow volume reference standard. The experiment was repeated for four stroke volumes ranging from 1–5ml. Furthermore, four healthy fetuses (gestational week 34-36) were included after informed consent by the mother-to-be. Data were acquired using a 1.5T MR system (Siemens Aera, Erlangen, Germany). A MOG-reconstructed PC-MRI sequence was used to estimate flow volumes and profiles in the umbilical vein after its entrance in the fetus and in the fetal descending aorta during a maternal breath hold. Typical sequence parameters: Voxel size 1.3x1.3x5mm3, velocity encoding 150cm/s, acquired temporal resolution 31ms and a simulated RR-interval of 525ms. Background phase correction was performed using subtraction of a first-order polynomial fit of the phase spatial variation for each acquisition. MOG reconstructions were performed in the MOG-OnIdea software (version 2.7) developed in Toronto. Flow curves and flow volumes with and without MOG reconstructions and reference methods were compared using Bland-Altman analysis for bias and variability, and the Wilcoxon matched-pairs signed rank test was applied with p<0.05 considered statistically significant.Results
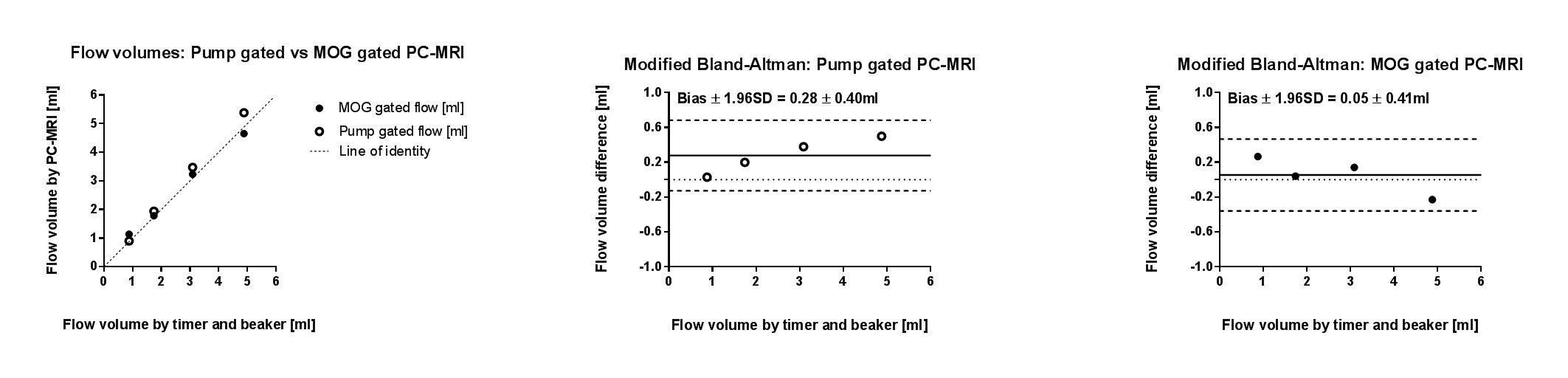
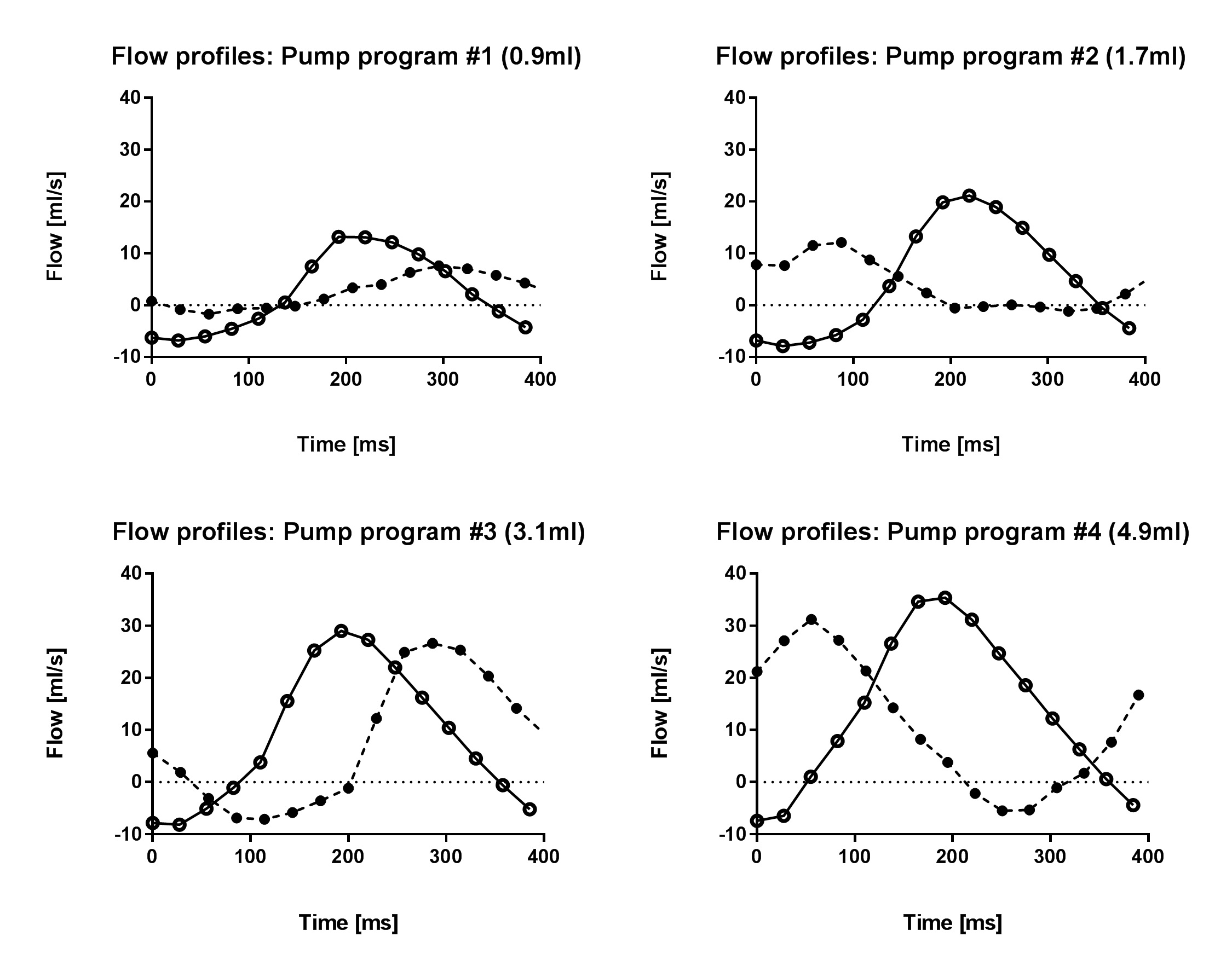
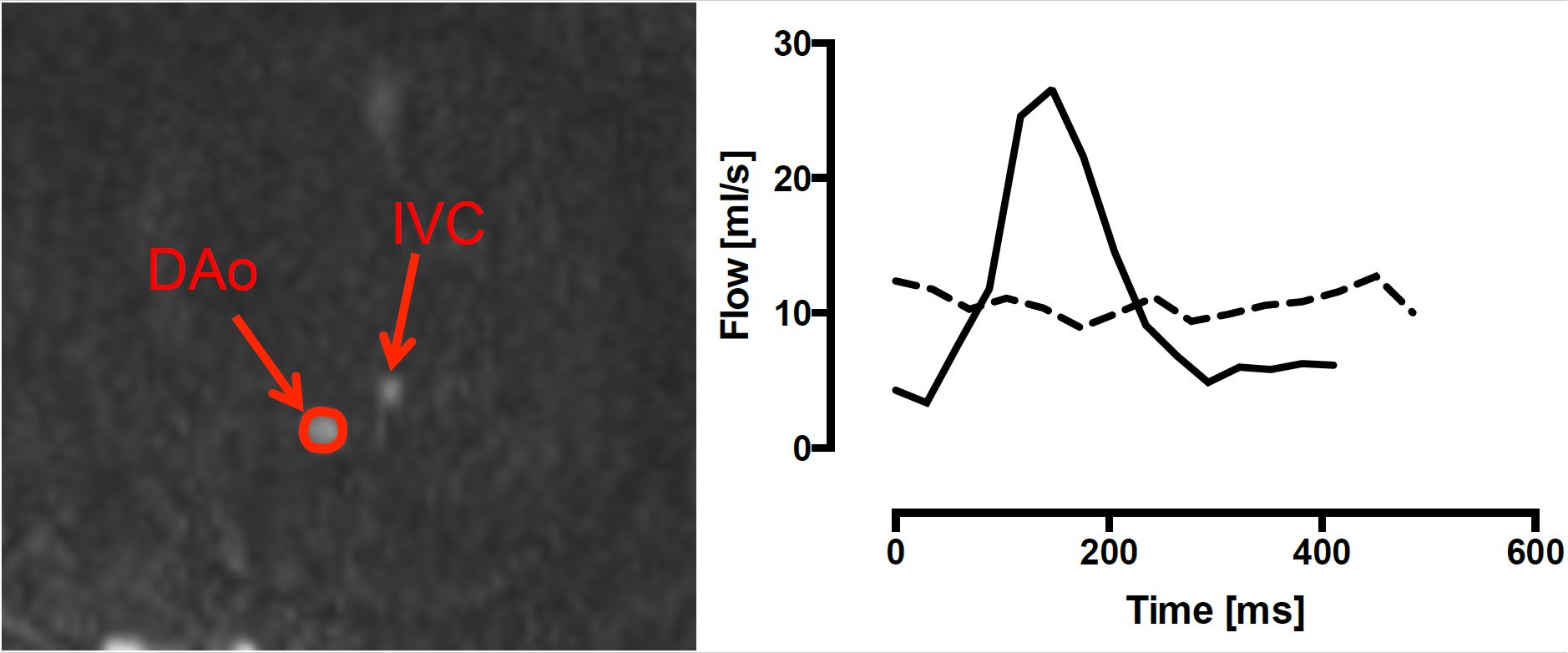
From timer/beaker measurements, the four pump programs delivered 0.9, 1.7, 3.1 and 4.9ml per pump stroke. PC-MRI showed pulsatile flow for all programs. Both pump- and MOG-gated acquisitions slightly overestimated flow volumes (0.3±0.4ml and 0.05±0.4ml, respectively; Figure 1). Figure 2 shows measured flow profiles from both sequences. MOG reconstructions underestimated peak flow rates compared to the pump-gated sequence for all programs. In the fetuses, vessel diameters of the umbilical vein and fetal descending aorta were 5–9mm. Flow pulsatility was not shown without MOG. After MOG reconstruction, pulsatile flow was shown in the descending aorta in all subjects (Figure 3). Stroke volume bias without and with MOG was 0.3±0.4 ml (umbilical vein;p=0.375) and -0.3±1.3 ml (descending aorta;p=0.75).Discussion
Phantom experiments showed overestimation of flow volumes by 2D PC-MRI. Residual background phase offsets connected to gradient hardware temperature variations as previously reported may explain this in part3. The reduced flow volume bias of the MOG sequence may originate from the observed underestimation of peak flow rates. Application of MOG in fetuses yielded pulsatile flow curves for the descending aorta but not for the umbilical vein, as expected in healthy pregnancies, and net flow volumes were preserved. Further optimization of the PC-MRI sequence in terms of spatial and temporal resolution may however improve measurements in smaller vessels, i.e. other vessels but also earlier during pregnancy or in growth-restricted fetuses.Conclusion
The pulsatile-flow phantom experiments show agreement between MOG PC-MRI, the reference gated sequence and timer/beaker flow volume measurements, while peak flow shows an underestimation which reproduces and confirms previous developments by Jansz et al1. In-vivo fetal flow quantification was feasible in a second center. This suggests MOG PC-MRI as a reliable tool for fetal cardiovascular flow quantification in more centers, increasing the availability of fetal cardiovascular MRI.Acknowledgements
No acknowledgement found.References
1. Jansz M, Seed M, van Amerom J, Wong D, Grosse-Worthmann L, Yoo SJ, Macqowan CK. Metric Optimized Gating for Fetal Cardiac MRI. Magn Reson Med. 2010;64(5):1304-1314.
2. Toger J, Bidhult S, Revstedt J, Carlsson M, Arheden H, Heiberg E. Independent Validation of Four-Dimensional Flow MR Velocities and Vortex Ring Volume Using Particle Imaging Velocimetry and Planar Laser-Induced Fluorescence. Magn Reson Med. 2016;75(3):1064-1075;
3. Busch J, Vannesjo J, Barmet C, Pruessmann K, Kozerke S. Analysis of temperature dependence of background phase errors in phase-contrast cardiovascular magnetic resonance. JCMR. 2014;97(16).
Figures