2828
Evaluate Systolic and Diastolic Wall Shear Stress of Aorta for Marfan Syndrome by 4D Flow MRIPin-Chen Chen1, Hsin-Hui Chiu2, Wen-Yih Isaac Tseng3, and Hsu-Hsia Peng4
1Institute of Systems Neuroscience, Hsinchu, Taiwan, 2Department of Pediatrics, Taipei, Taiwan, 3Institute of Medical Device and Imaging, Taipei, Taiwan, 4Department of Biomedical Engineering and Environmental Sciences, Hsinchu, Taiwan
Synopsis
We aim to reveal the abnormality of plane-wise and segmental WSS in different cardiac phases of patients with Marfan syndrome (MFS) with dilated aorta. MFS group presented lower plane-wise axial WSS than normal group at ascending aorta and descending aorta during systole. In respect of segmental WSS, either in the whole cardiac cycle or during systole, MFS patients demonstrated reduced values at almost all segments in proximal ascending aorta. In conclusion, the quantitative indices of plane-wise and regional WSS clearly differentiate MFS patients from normal controls. Therefore, quantification of WSS can provide promising approaches for patient managements in the future.
Introduction
Cardiovascular systems are thought to be affected in patients with Marfan syndrome (MFS). In previous studies, wall shear stress (WSS) and helical flow were reported to have impact on endothelial cell function and gene expression [1, 2]. Therefore, for MFS patients with dilated aortic root, it is important to evaluate their vessel wall functions by calculating velocity- and WSS-related parameters. Geiger et al measured the plane-wise time-averaged WSS and reported that there is no significant difference between asymptomatic MFS patients and normal controls. Wang et al demonstrated lower time-averaged WSS in MFS patients with dilated aorta [3]. In this study, we quantified plane-wise axial WSS separately in systole and diastole along the aorta of MFS patients. We also analyzed the segmental WSS to detect the regional abnormality of WSS on the aortic wall. The purpose is to reveal the abnormality of plane-wise as well as segmental WSS in different cardiac phases of MFS patients with dilated aorta.Methods
The study population recruited 15 normal subjects (age = 25.0 ± 7.1 years; female/male = 7/8) and 18 MFS patients (age = 29.0 ± 10.6 years; female/male = 6/12). All measurements were performed on a 3 Tesla system (Tim Trio, Siemens, Erlangen, Germany). The aortic root diameter in the sinuses of Valsalva was estimated on cine SSFP images at peak systole. Aortic flow was assessed using 4D phase-contrast MRI (PC-MRI). Scanning parameters were as follows: TR/TE = 10/2.7 ms, flip angle = 7˚, temporal resolution = 40 ms, spatial resolution = (1.36-1.44) × (1.36-1.44) × 3.5 mm3, and venc = 1.5 m/s in three directions. The 3D blood flow visualization was achieved by reconstructing a 3D PC MR angiogram (MRA) from 4D flow data in a commercial software (EnSight 9.2, CEI Inc., Apex, NC). Fourteen 2D planes along the aorta were manually placed on the MRA and were perpendicular to long axis of aorta (Figure 1). Axial WSS = 𝝁×𝒅𝒖/𝒅𝒓, where 𝝁 = viscosity, u = velocity along the vessel axis, and r = distance perpendicular to and away from the wall. Statistical analysis was performed by using Student’s t-test, and multiple comparison was also be considered. A P value < 0.05 was considered statistically significant.Results
Table 1 illustrates the demographics of the study population. MFS group was with larger aortic root diameter than normal group (38.9 ± 8.9 mm vs. 25.9 ± 4.5 mm, P < 0.05). In Figure 2, MFS group presented lower plane-wise axial WSS than normal group at ascending aorta (AAo planes 1-4) and descending aorta (DAo, plane 12 and plane 14) during systole. There was no significant difference between two groups on the plane-wise diastolic WSS. In respect of reginal WSS, either in the whole cardiac cycle or solely during systole, MFS patients demonstrated reduced values at almost all segments in plane 1 to plane 3 (Figures 3). However, during diastole, there was no significant difference between the two groups (Figure 4).Discussions and conclusions
Geiger et al proved that WSS played an important role in evaluating the function of the aortic wall in asymptomatic MFS patients [2]. They reported that plane-wise time-averaged WSS showed no significant difference between asymptomatic MFS patients and normal controls and higher segmental WSS at peak systole was demonstrated in MFS group. However, our findings, displaying lower WSS values in both of plane-wise WSS as well as in segmental WSS, is inconsistent to the previous study. It can be attributed to that the MFS in Geiger’s study were young and with lower BSA, potentially resulted in decreased flow rates and thus lower peak systolic WSS. In conclusion, the quantitative indices of plane-wise and regional WSS clearly figured out the difference between normal subjects and MFS patients. Therefore, quantification of WSS can provide promising approaches for patient managements in the future.Acknowledgements
No acknowledgement found.References
1. Geiger et al, J Magn Reson Imaging. 2012, 35:594-600. 2. Geiger et al, Magn Reson Med. 2013, 70(4):1137-44. 3. Wang et al, J Magn Reson Imaging. 2016, 44(2):500-8.Figures
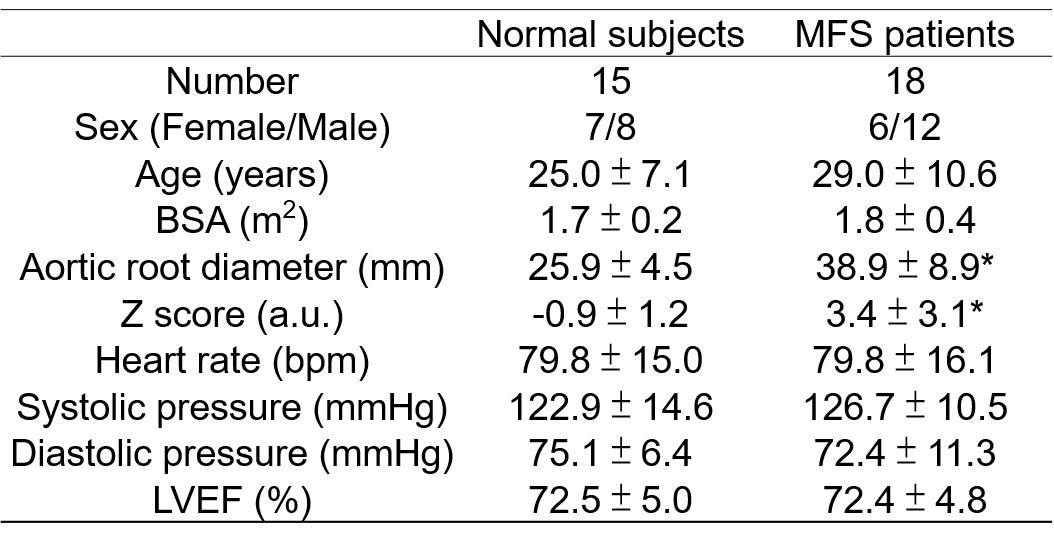
Demographics of the study population.
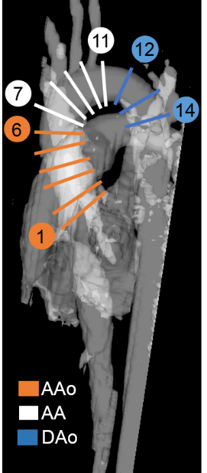
The manually determined 14 2D planes for computing hemodynamics.
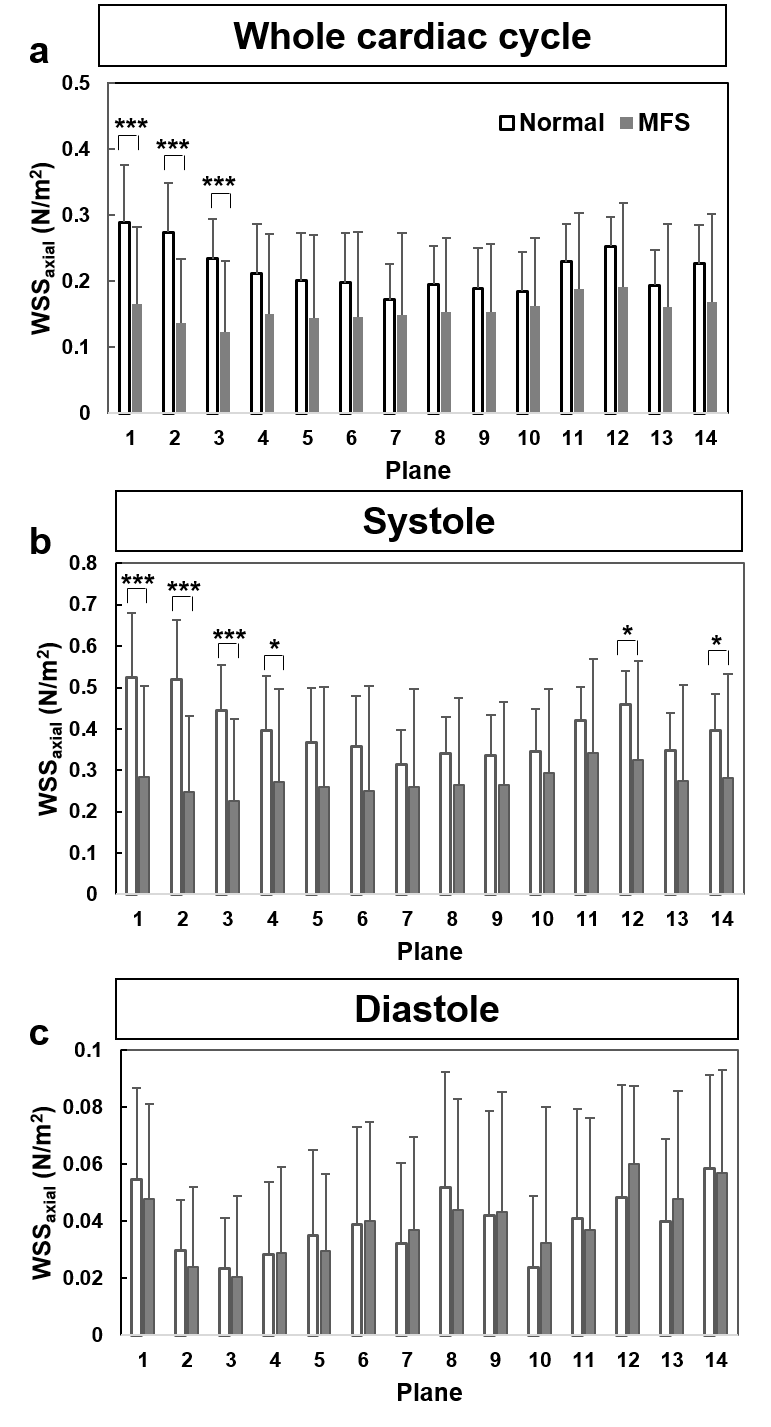
Axial WSS of normal and MFS groups during (a)
whole cardiac cycle, (b) systole, and (c) diastole. *P < 0.05, ***P <
0.001.
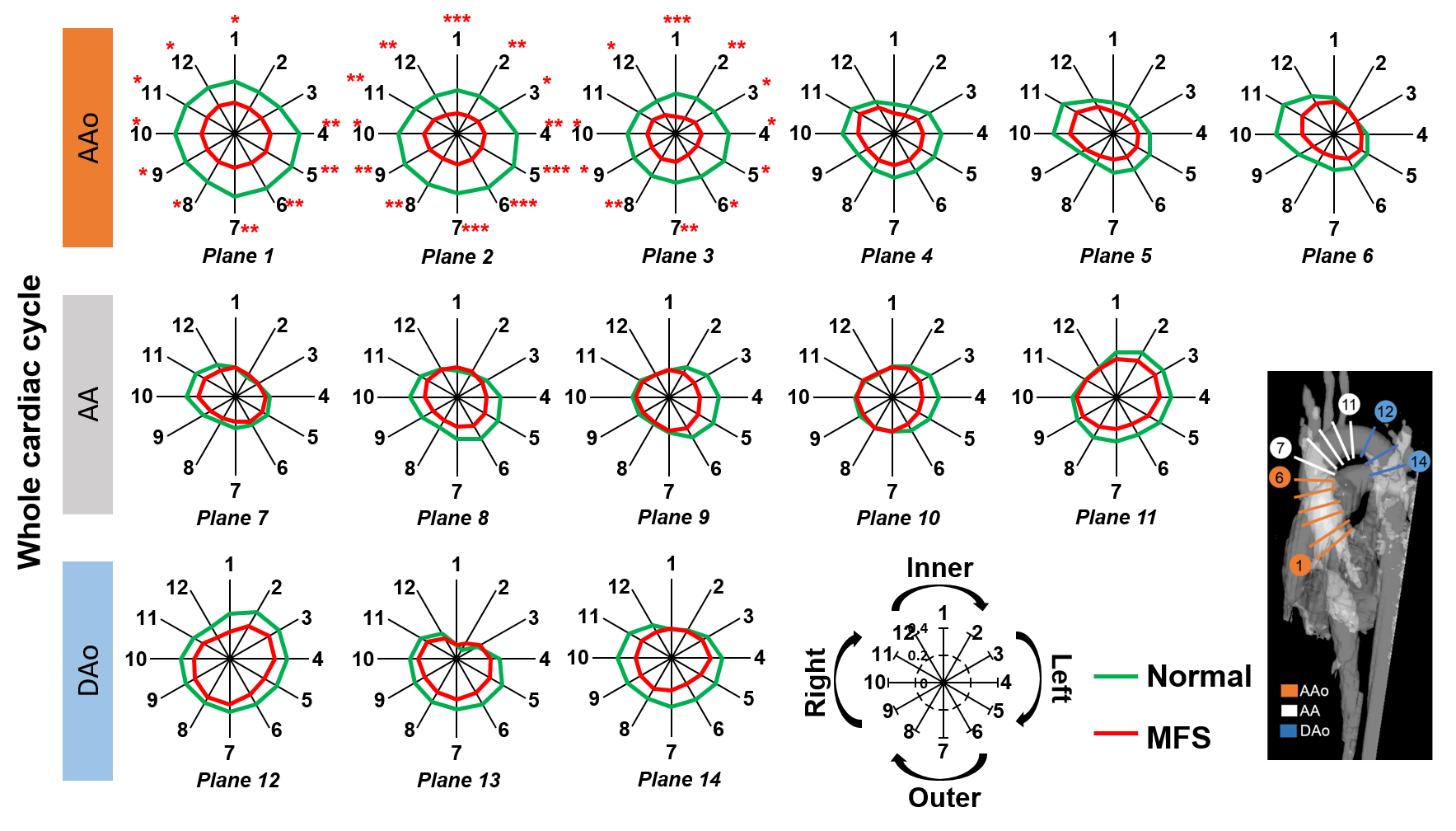
Segmental axial WSS of normal (green line) and
MFS groups (red line) in ascending aorta (AAo), aortic arch (AA), and
descending aorta (DAo) during whole cardiac cycle. *P < 0.05, **P < 0.01,
***P < 0.001.
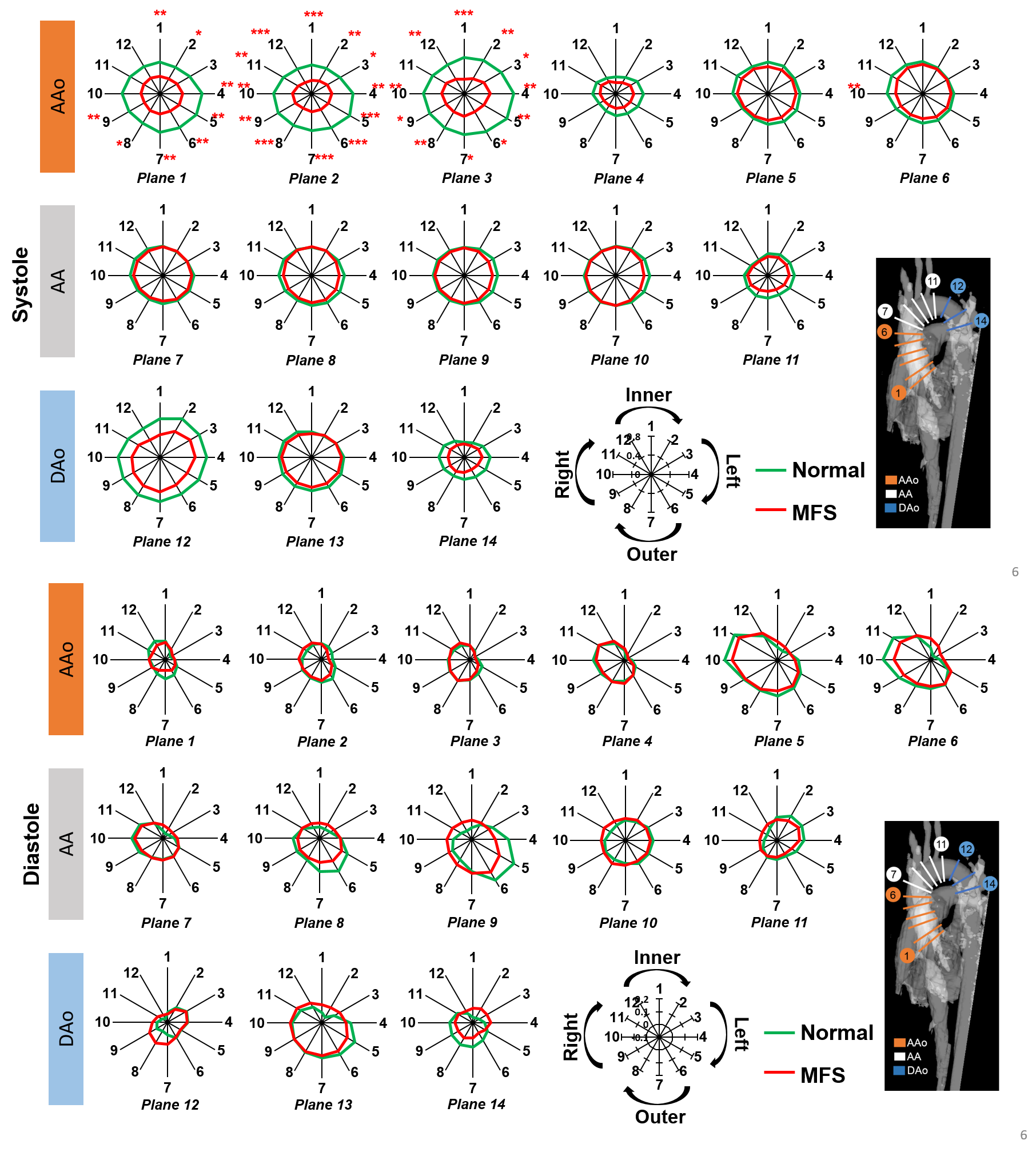
Segmental axial WSS of normal (green line) and
MFS groups (red line) in ascending aorta (AAo), aortic arch (AA), and
descending aorta (DAo) during systole and diastole. *P < 0.05, **P < 0.01,
***P < 0.001.