2813
A Novel Technique for 4D Time-of-Flight MR Angiography using Double Adiabatic Inversion Recovery Pulses1Department of Radiology, Tokai University Hospital, Kanagawa, Japan, 2Healthcare department, Philips Electronics Japan, Tokyo, Japan, 3Graduate School of Medical Sciences, Kanazawa University, Kanazawa, Japan, 4Department of Radiology, Tokai University Hachiouji Hospital, Tokyo, Japan, 5Radiology, Tokai University School of Medicine, Kanagawa, Japan
Synopsis
Although previously developed 4D time-of-flight (4D-TOF) at a 3T MR system for evaluating cerebral hemodynamics, this method did not fit at a 1.5T MR system in order to early recovery the brain tissue signals. We proposed a novel 4D-TOF technique using double adiabatic inversion recovery pulse (DIR 4D-TOF) for suppressing background recovery and depiction of intracranial artery at a 1.5T MR system. The results presented show that DIR 4D-TOF with long interval between the first and the second adiabatic inversion recovery pulses could effectively delay T1 recovery of the brain tissue and improved visibility of intracranial artery.
PURPOSE
4D time-of-flight (4D-TOF) magnetic resonance angiography (MRA) has been introduced as a technique for time-resolved MRA at a 3T MR system without the arterial spin labeling (ASL) technique1. 4D-TOF can be acquired with saturation pulses, and thus does not require subtraction of images. This technique can provide high-quality images to observe the intracranial hemodynamics and allow faster acquisition without misregistration artifact. Meanwhile, 1.5T MR systems still have the highest market share in clinical practice2 and can be available for patients with metallic implants. However, the original 4D-TOF may not be suitable at a 1.5T MR system for clear depiction of the intracranial arteries due to the signal recovery of the brain tissue particularly in the late phase because T1 relaxation time is shorter at a 1.5T MR system than at a 3T MR system3. The purpose of this study was to assess a novel 4D-TOF MRA technique using double adiabatic inversion recovery pulse (DIR 4D-TOF) for depiction of the intracranial arteries at a 1.5T MR system.METHODS
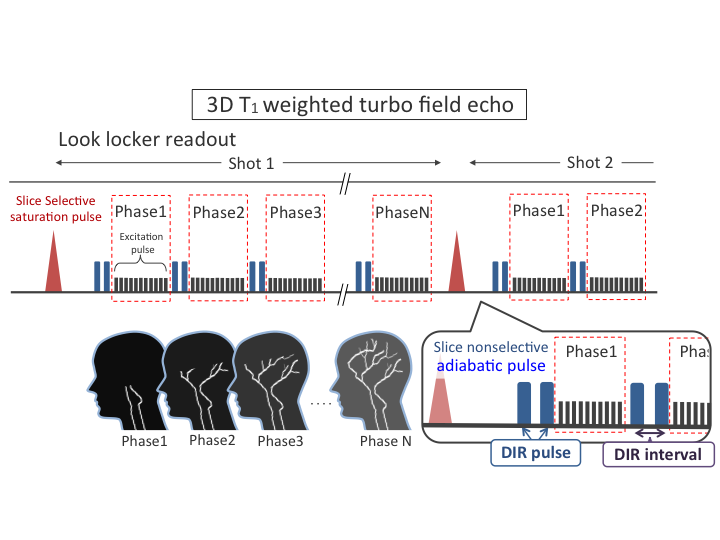
DIR 4D-TOF sequence (Figure 1) employed 3D T1 weighted turbo field echo (TFE) sequences by the inflow effect combined with Lock–Locker readout. In this sequence, a slice-selective saturation pulse was applied at the first part of the sequence to suppress all tissue. We applied double inversion recovery (DIR) pulse using a slice nonselective adiabatic pulse prior to each phase encoding to delay the signal recovery of the brain tissue. DIR interval was defined as the interval between the first and the second adiabatic inversion recovery pulses. Data was collected in 6 healthy volunteers (6 males; mean age, 27.7 ± 4.8 years; age range, 24–38 years) by using original 4D-TOF and DIR 4D-TOF with DIR intervals of 10, 30 and 50 msec at a 1.5T MR system (Achieva; Philips Healthcare). The parameters of DIR 4D-TOF images were as follows: FOV = 200 × 200 mm2, acquired resolution = 1.0 × 1.3 × 1.0 mm3, reconstructed resolution = 0.5 × 0.5 × 1.0 mm3, TR = 8 msec, TE = 2.1 msec, parallel imaging factor = 2.5, temporal resolution = 255 msec, temporal phase = 6 phases from 40 to 1317 msec, and scan time = 4.7 min. The original 4D-TOF images were same parameters except for the use of DIR. The signal of the white matter on each sequence were measured in each temporal phase, and the signal intensity ratios (SIR) of the signal at phase2–6 to that at phase1 were calculated as an indicator of the suppression effect in each sequence. Then, a neuroradiologist (17 years of experience) and a radiologist (16 years of experience) in clinical neuroimaging assessed the visibility of distal branches (M4) on the maximum intensity projection (MIP) of the last temporal phase in random order in a blinded manner on each sequence. The visual evaluation of M4 was independently rated by two radiologists using a five-point scale: 1 = poor (non-diagnostic), 2 = fair (observer not confident), 3 = moderate (observer marginally confident), 4 = good (observer confident), and 5 = excellent (observer highly confident). The M4 visibility scores were compared using the Friedman test among the sequence.RESULTS and DISCUSSION
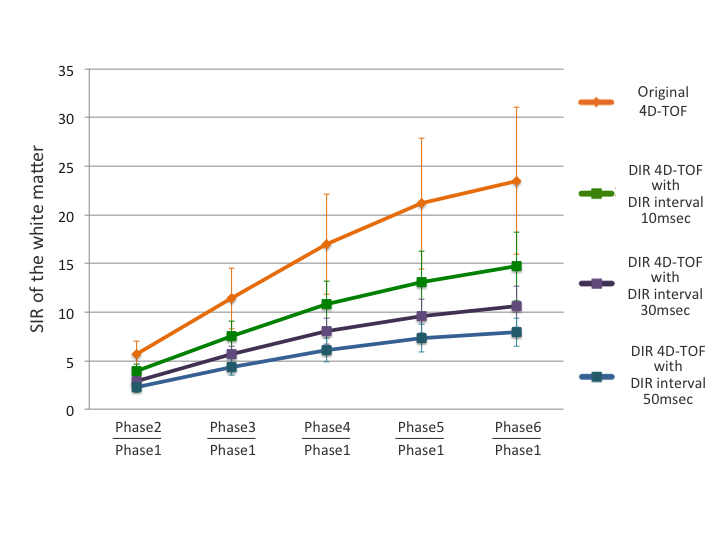
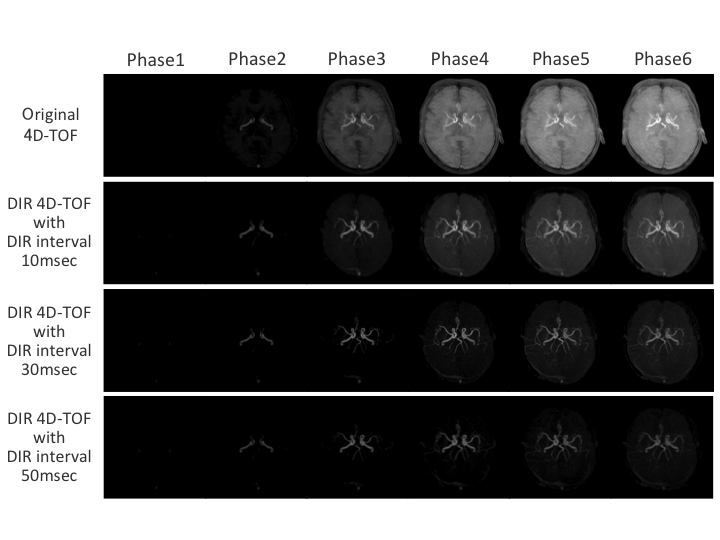
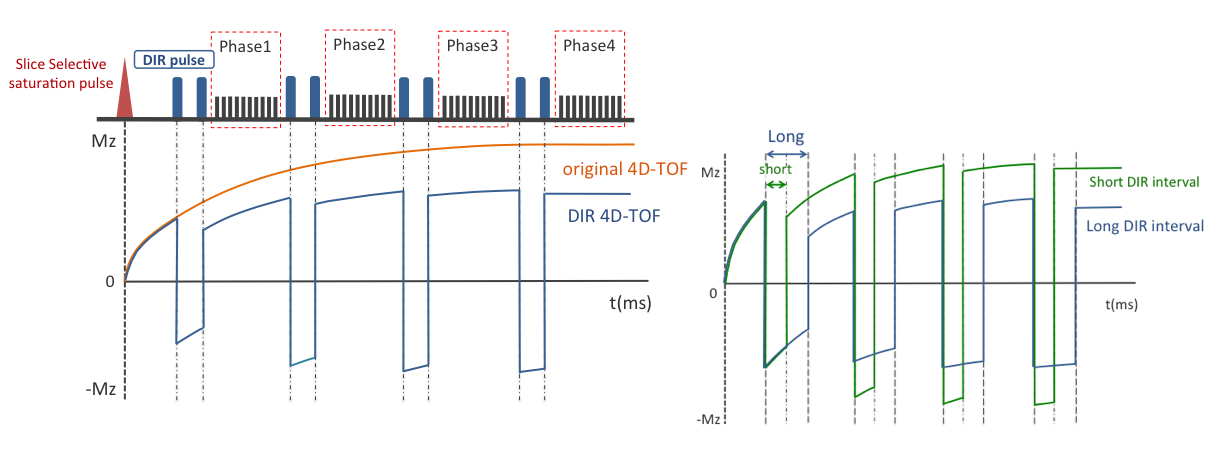
SIR curves at temporal phases on each sequence are shown in Figure 2. Compared with the other sequence, the signal in the white matter was slowly recovered and was smaller in the last phase on DIR 4D-TOF with DIR interval 50msec. The MIP images of each sequence for a subject are shown with the same window level in Figure 3. In this figure, DIR 4D-TOF with DIR interval 30 and 50 msec images provided good visualization of M4 in the last phases. The mean score was 1.17 (standard deviation (SD) = 0.37) for original 4D-TOF, 3.17 (SD = 0.69) for DIR 4D-TOF with DIR interval 10 msec, 3.58 (SD = 0.76) for DIR 4D-TOF with DIR interval 30msec, and 4.33 (SD = 0.74) for DIR 4D-TOF with DIR interval 50 msec which achieved the highest M4 visibility. There was a significant difference among each sequence for both readers (P < 0.001). These results suggest that DIR 4D-TOF with long DIR interval can effectively delay T1 recovery of the brain tissue (Figure 4) and improve visibility of the intracranial artery, compared with the original 4D-TOF at a 1.5T systems.CONCLUSION
DIR 4D-TOF with long DIR interval improved depiction of the intracranial arteries at a 1.5T MR system.Acknowledgements
No acknowledgement found.References
1. Shibukawa S et al. Optimized 4D time-of-flight MR angiography using saturation pulse. J Magn Reson Imaging. 2016;43(6):1320-6.
2. Kraff O et al. MRI at 7 tesla and above: demonstrated and potential capabilities. J Magn Reson Imaging. 2015;41(1):13-33.
3. Ethofer T et al. Comparison of longitudinal metabolite relaxation times in different regions of the human brain at 1.5 and 3 tesla. Magn Reson Med. 2003;50(6):1296-301.
Figures