2812
Non-contrast enhanced MR angiography of lower extremity in patients with diabetes: initial experience of using TRANCE technique at 3.0 T1MRI, The 1st affiliated hospital of Henan University of TCM, ZhengZhou, People's Republic of China, 2ShenZhen Institutes of Advanced Technology, People's Republic of China
Synopsis
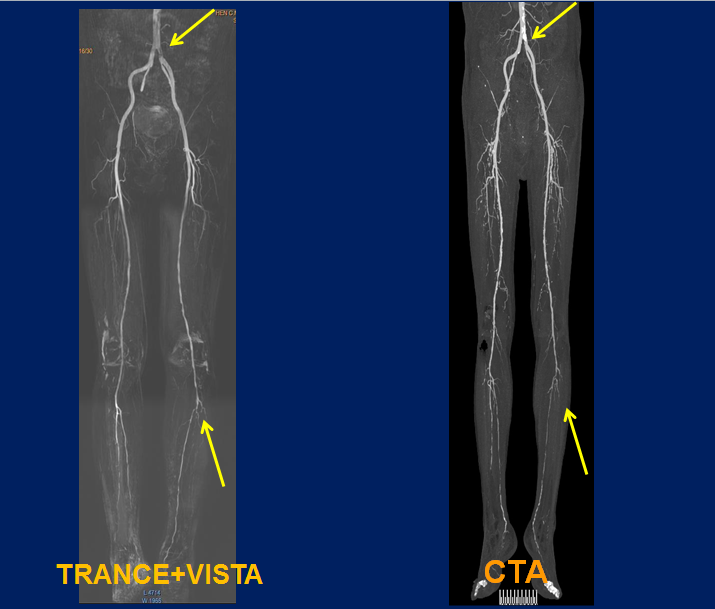
There is a clinical need for implementing a Non-contrast enhanced imaging technique for patients with peripheral arterial disease or diabetes and contraindications for the use of contrast medium, especially patients with decline in kidney function or renal artery stenosis. We optimized TRANCE technique combined with VISTA for best performance of NCE-MRA for lower extremity artery at 3.0T MRI.
Introduction
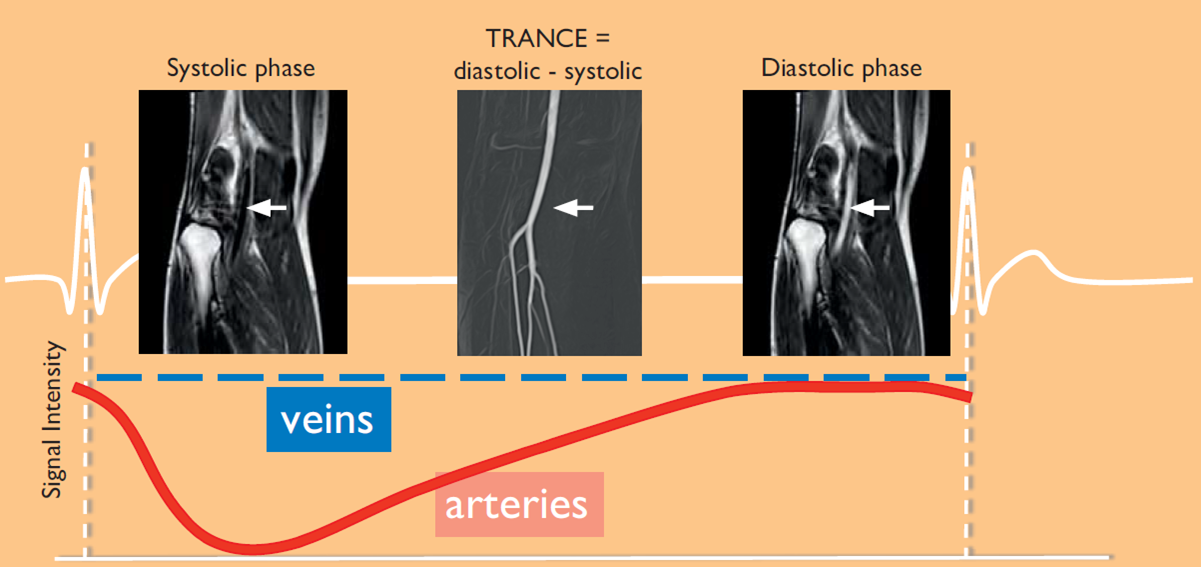
Contrast-enhanced MR angiography (CE-MRA) has become a noninvasive modality of choice for detecting arterial disease of lower extremities. However, patients with renal insufficiency who receive contrast agents will be at the risk of nephrogenic systemic fibrosis (NSF) related to gadolinium-based contrast agents. Non-contrast enhanced MR angiography (NCE-MRA) gained more clinical interest and MR imaging without gadolinium-based contrast agents is preferred. Conventional NCE-MRA techniques based on time-of-flight and phase-contrast are not widely applied in lower extremities, primarily due to limited time efficiency, slow flow, or potential image artifacts. TRANCE (Triggered Angiography Non-Contrast Enhanced) is a cardiac triggered 3D TSE technique that subtracts images from different phases in the cardiac cycle to obtain high resolution arterial images with bright vessels and dark background. TRANCE technique has been optimized for best performance at 1.5T, but seldom used at 3.0T because of acquisition by surface coil instead of body matrix coil at 3.0T. This study we improved and optimized TRANCE technique for better demonstration of NCE-MRA for lower extremity artery.Methods
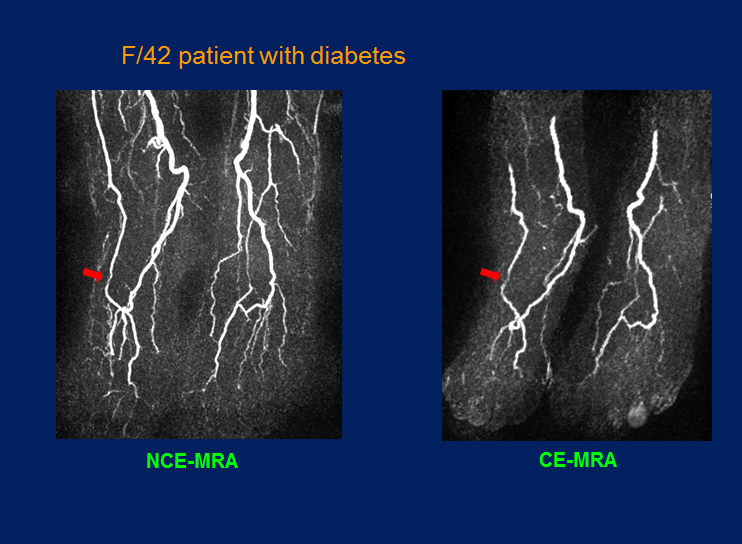
A total of 45 patients with diabetes according to 2006 WHO diabetes criteria performed both NCE-MRA and CE-MRA examination for bilateral distal lower extremity. MRA were performed on 3.0 T (Ingenia, PHILIPS, Netherlands) with surface coil. TRANCE technique uses cardiac triggering to enable data acquisition during systole and during diastole, which subtracts these two high resolution datasets, resulting in only arterial signal as the bright signal of the veins is cancelled out. Thus flow changes throughout the cardiac cycle are used to better differentiate arteries from background tissue. We combined TRANCE and VISTA (volume isotropic turbo spin echo acquisition) for best performance of full fat suppression. The parameters for TRANC: TR/TE 1.8ms/3.3ms,NSA 1,FOV 380mm×380mm,thickness 1.1mm,Flip angle 90°, receiver bandwidth 965 Hz/pixel. CE-MRA was performed with a 3D gradient-echo sequence. Relevant parameters included: TE/TR 1/3ms, flip angle 25°, thickness 1.2 mm, FOV 320×320 ,matrix size 256×256.
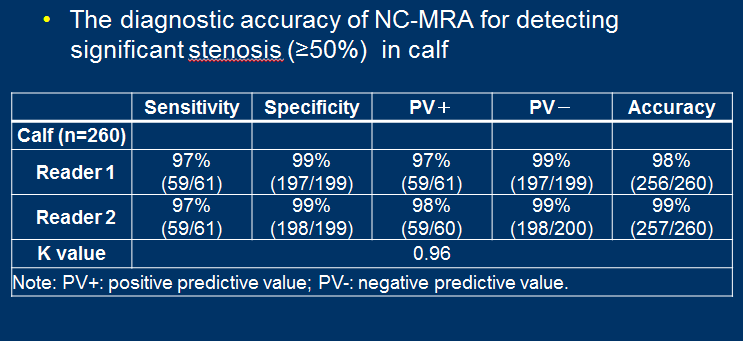
Image quality was evaluated on three calf arterial segments. Each arterial segment was rated on a 4-point scale. An image quality score of 2 to 4 was defined as diagnostic image quality. Arterial blood signal to-noise ratio (SNR) and artery-tissue contrast-to noise ratio (CNR) were calculated for both NCE-MRA and CE-MRA. To compare NCE-MRA with CE-MRA, a Wilcoxon signed rank test was performed for determining the difference in image quality. The diagnostic sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of NCE-MRA for detecting significant stenosis were calculated on segmental and patient’s basis using CE-MRA as the reference standard. Cohen’s kappa statistic was used to evaluate inter-observer agreement for assessing significant arterial stenosis on NCE-MRA.
Results
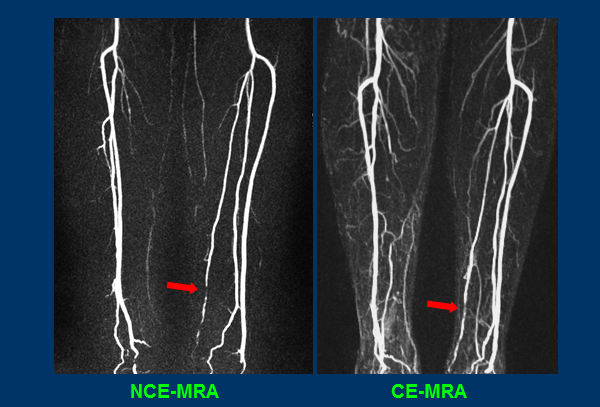
There was no significant difference in the number of diagnostic arterial segments between the two techniques for NCE-MRA and CE-MRA. Image quality of CE-MRA was slightly higher than that of NCE-MRA (P < 0.01). With the high isotropic spatial resolution and high artery-tissue CNR, NCE-MRA demonstrated excellent performance for the delineation of luminal narrowing and small collateral arteries that were consistent with CE-MRA. Quantitative analysis shows that SNR and CNR of NCE-MRA are significantly higher than those of CE-MRA (P<0.01). The average sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of NCE-MRA were 97%, 96%, 90%, 99%, and 96%, respectively, on a per-segment basis and 90%, 84%, 82%, 91%, and 87%, respectively. The kappa value for inter-observer agreement between the two readers was 0.96.Discussion
TRANCE makes use of signal intensity differences in the arteries due to flow changes throughout the cardiac cycle. TRANCE background suppression is mostly excellent at 1.5T and it could be very easily see collateral blood circulation. TRANCE is compatible with large FOV (380 to 450 mm) and high matrix sizes with scan time faster than TOF. But TRANCE background suppression is not sufficient and homogeneous at 3.0T. We have optimized scan parameters, such as refocusing angle and flow compensation, especially combined with VISTA technique. VISTA can help to enhance subtraction and fat suppression much more fully. Now it realized NCE-MRA with best demonstration for lower extremity arteries with TRANCE and VISTA at 3.0T.Conclusion
NCE-MRA using TRANCE technique demonstrated adequate image quality in the delineation of lower extremity arteries and consistent diagnostic performance for detecting significant stenosis with CE-MRA in patients with diabetes. It provides a good alternative to CE-MRA for the evaluation of calf arterial disease in diabetic patients with renal insufficiency or those who are preferred non-contrast agent examination.
Acknowledgements
Contract grant sponsor: Traditional Chinese Medicine Research Project of Henan Province of China. Contract grant number: 2015ZY02014References
1 Wheaton AJ, Miyazaki M. Non-contrast enhanced MR angiography: physical principles. J Magn Reson Imaging 2012;36:286–304.
2 Bonel H M, Saar B, Hoppe H, et al. MR Angiography of Infrapopliteal Arteries in Patients with Peripheral Arterial Occlusive Disease by Using Gadofosveset at 3.0 T: Diagnostic Accuracy Compared with Selective DSA 1[J]. Radiology, 2009, 253(3): 879-890.
3 Fan Z, Sheehan J, Bi X, et al. 3D noncontrast MR angiography of the distal lower extremities using flow-sensitive dephasing (FSD)-prepared balanced SSFP[J]. Magnetic resonance in medicine, 2009, 62(6): 1523-1532.
4 Miyazaki M, Takai H, Sugiura S, et al. Peripheral MR Angiography: Separation of Arteries from Veins with Flow-spoiled Gradient Pulses in Electrocardiography-triggered Three-dimensional Half-Fourier Fast Spin-Echo Imaging 1[J]. Radiology, 2003, 227(3): 890-896.
5 Offerman E J, Hodnett P A, Edelman R R, et al. Nonenhanced methods for lower-extremity MRA: A phantom study examining the effects of stenosis and pathologic flow waveforms at 1.5 T[J]. Journal of Magnetic Resonance Imaging, 2011, 33(2): 401-408.
6 Liu X, Fan Z, Zhang N, et al. Unenhanced MR angiography of the foot: initial experience of using flow-sensitive dephasing–prepared steady-state free precession in patients with diabetes[J]. Radiology, 2014, 272(3): 885-894.
7 Wheaton A J, Miyazaki M. Non-contrast enhanced MR angiography: Physical principles[J]. Journal of Magnetic Resonance Imaging, 2012, 36(2): 286-304.
8 Fan Z, Hodnett PA, Davarpanah AH, et al. Non-contrast magnetic resonance angiography of the hand: improved arterial conspicuityby multidirectional flow-sensitive dephasing magnetization preparation in 3D balanced steady-state free precession imaging. Invest Radiol 2011;46:515–523.
Figures