2811
Can non-contrast Fresh Blood Imaging (FBI) provide sufficient pretreatment information of peripheral artery disease (PAD)?1Department of Radiology, Saiseikai Kumamoto Hospital, Kumamoto, Japan, 2Department of Cardiovascular, Saiseikai Kumamoto Hospital, Kumamoto, Japan, 3Department of Radiology, Kumamoto city Hospital, Kumamoto, Japan, 4Department of Radiology, Tobata Kyoritsu Hospital, Fukuoka, Japan, 5Toshiba Medical Research Institute USA, Japan
Synopsis
Diagnostic accuracy of nonenhanced Fresh Blood
Imaging (FBI) was compared with digital subtraction angiography (DSA) or digital
angiography (DA), which was performed at percutaneous transluminal angioplasty (PTA), in the evaluation of
the peripheral lower-extremity arteries. In the evaluation of 173 segments
in 25 patients with peripheral arterial occlusive disease, the sensitivity,
specificity, and accuracy of FBI of a consensus reading for detection of 50%
or greater stenotic lesions were 100%, 83%, and
88%, respectively. FBI achieves
high diagnostic accuracy for the detection of peripheral arterial disease (PAD)
in comparison with DSA.
PURPOSE
Fresh blood imaging (FBI) is a novel non-enhanced 3D MR angiography technique, using a physiological signal change of an artery during a cardiac cycle1), 2). Diagnostic capability of FBI using appropriate read-out gradients on peripheral arterial disease (PAD) was reported to be comparable with that of 16 detector-row CT angiography3); however, the comparison with conventional x-ray angiography as a gold standard has not been reported for the diagnosis of PAD. Because conventional x-ray angiography is recommended for evaluation of patients with PAD when revascularization is contemplated4), it might be difficult to perform for diagnostic purpose. The purpose of study is to compare FBI with digital subtraction angiography (DSA) or digital angiography (DA), which was performed at percutaneous transluminal angioplasty (PTA), in the evaluation of the peripheral lower-extremity arteries.
METHODS
A total of 25 patients (19 men and 6 women [50 – 88 y.o., mean, 69 y.o.]) with PAD from October 2006 to October 2015, was included in this study. All patients underwent both FBI and DSA/DA examinations within one month (range, 1-25 days; mean, 14 days). For data analysis, the arterial vascular system was divided into 15 anatomic segments (infrarenal aorta, right and left common iliac, external iliac, superficial femoral, popliteal, anterior tibial, posterior tibial, and peroneal arteries). DSA/DA was performed only for the purpose of PTA on the patients who were suspected PAD by FBI; only unilateral side of lower limb stenotic arteries was examined by DSA/DA in 20 of 25 cases and arteries of both limbs were examined in 5 cases. A total of 173 segments was evaluated in this study. Each segment of FBI was evaluated independently by two observers; a board-certified radiologist with 20 years of clinical experience and a board-certified cardiologist with 15 years of clinical experience, using a five-point grading system (grade 1, <10% luminal narrowing; grade 2, 10%-49%; grade 3, 50%-74%, grade 4, 75-99%; and grade 5, occlusion). When the evaluation results of two observers were different, the final score was reached with a consensus reading by the two. The DSA/DA was evaluated by the cardiologist using the same grading system by using static and dynamic images. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy for detection of stenotic lesions using FBI were calculated, with findings on DSA as the gold reference standard. All MR examinations were performed using a 1.5-T clinical imager (EXCELART Vantage XGV; Toshiba Medical, Tochigi, Japan) using a torso SPEEDER coil. Three-dimensional (3D) half-Fourier FSE acquisition parameters were as follows: TR= 3-4 RR intervals, TEeff =80 msec, TI=150 msec, ETS= 5 msec, matrix=256 x 256, section thickness = 4 mm (interpolated to 2 mm), FOV = 38 x 38 cm, and an acquisition time of 2-3 minutes per station. The appropriate read-out spoiler gradients were applied accordingly to each station3). The suitable diastolic and systolic ECG delay times were determined by ECG preparation scan. After acquisition, the systolic source images were subtracted from the diastolic source images, and the subtracted images underwent MIP processing. Angiography examinations were performed with Image Intensifier angio system, or flat panel system (infinix celeve; Toshiba Medical, Tochigi, Japan).RESULTS
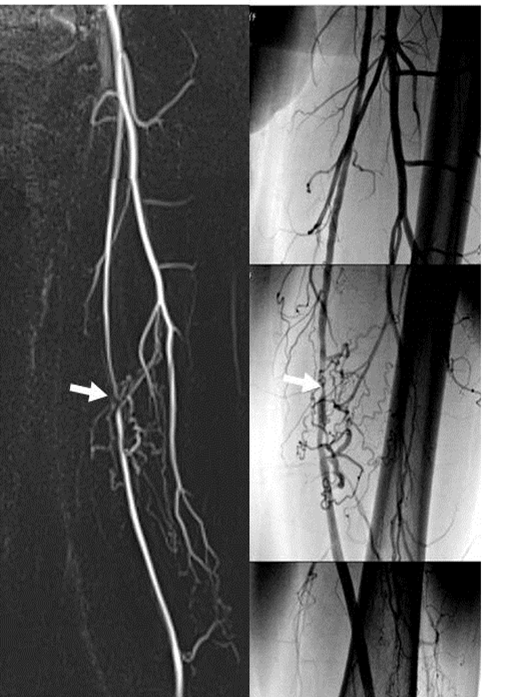
DSA/DA identified significant stenosis in 52 of 173 segments; 26 with severe stenosis, and 26 with occlusion. The sensitivity, specificity, PPV, NPV, and accuracy of FBI by the consensus reading with regard to detection of 50% or greater luminal reduction, indicating hemodynamically significant stenosis, were 100%, 83%, 72%, 100%, and 88%, respectively (Table1). Typical comparison images of FBI and DSA were shown in Figure 1.DISCUSSION
The cardiologist evaluated relatively a low sensitivity (88%) and a high specificity (89%); whereas, the radiologist assessed the high sensitivity (100%) and the low specificity (67%). Each observer indicated different characteristics in the stenotic reading; however, the consensus reading improves to a higher performance than that of average score of each observer. The stenotic segments, which were evaluated as not significant by the cardiologist, were the stenosis slightly over 50%. The false positive detection by the radiologist were observed in oblique portions, in which flow turbulence tended to occur after the stenosis. Limitation of this study was that DSA/DA underwent only for the diseased side for the PTA in the most of the cases; therefore, there were relatively small number of mild or moderate stenosis, which might affect the lower specificity.CONCLUSION
FBI achieves
high diagnostic accuracy for the detection of PAD in comparison with DSA,
especially reaching with the consensus reading by pleural observers. The
FBI technique is a non-invasive, non-contrast-enhanced,
high-confident, and cost-effective method for the evaluation of PAD.
Acknowledgements
No acknowledgement found.References
1) Miyazaki M, Takai H, Sugiura S, et al. Radiology 227:890-896, 2003.
2) Miyazaki M, Lee VS. Radiology 248: 20-43, 2008.
3) Nakamura K, Miyazaki M, Kuroki K, et al. MRM. 65(2):595-602, 2011.
4) ACC/AHA 2005 Practice Guidelines for the Management of Patients With Peripheral Arterial Disease (Lower Extremity, Renal, Mesenteric, and Abdominal Aortic) Circulation. 2006;113: e463-e654
Figures

Table1: Performance of FBI compared with DSA