2805
Breath-hold and Free-Breathing Single-Shot Radial Quiescent-Interval Slice-Selective (QISS) MRA for Evaluation of the Pulmonary ArteriesRobert R. Edelman1,2, Shivraman Giri3, Robert Silvers1, Kiran Thakrar1, and Ioannis Koktzoglou4,5
1Radiology, NorthShore University HealthSystem, Evanston, IL, United States, 2Radiology, Northwestern University, Chicago, IL, United States, 3Siemens HealthCare, 4Radiology, NorthShore University HealthSystem, 5Radiology, University of Chicago
Synopsis
For suspected pulmonary embolism, CTA is the first-line imaging test, with CEMRA a potential alternative. Disadvantages including exposure to ionizing radiation and iodine contrast for CTA, while CEMRA is sensitive to respiratory motion and requires a gadolinium-based contrast agent. As a nonenhanced alternative, we tested breath-hold and free-breathing versions of single-shot radial QISS. Compared with the reference standard, all pulmonary artery branches down to the segmental level were visualized by breath-hold and navigator-gated QISS. With further optimization and validation, radial QISS has the potential to provide a nonenhanced alternative to CTA and CEMRA for the evaluation of suspected pulmonary embolism.
Purpose:
For patients presenting to the emergency department with chest pain, one of the most important considerations in the differential diagnosis is pulmonary embolism. Pulmonary embolism causes tens of thousands of deaths annually and has a 20% 90-day mortality rate. Unfortunately, the symptoms are non-specific, so that imaging is often required to make an accurate diagnosis. CT angiography has replaced the radionuclide ventilation-perfusion scan as the mainstay of diagnosis (1). While CTA provides accurate evaluation of the pulmonary arteries, it exposes patients to ionizing radiation and requires iodine contrast administration, which is contraindicated in patients with impaired renal function. Contrast-enhanced MR angiography (CEMRA) of the pulmonary arteries is a potential alternative (2). While eliminating radiation exposure, it requires the administration of a gadolinium-based contrast agent which is contraindicated in patients with impaired renal function as well as in pregnant women. Moreover, CEMRA requires a lengthy breath-hold, which may not be feasible if the patient is dyspneic as is common in pulmonary disorders such as pulmonary embolism. We therefore explored the feasibility of applying nonenhanced MRA techniques to depict pulmonary arterial anatomy, using breath-hold and free-breathing implementations of single-shot radial quiescent-interval slice-selective (QISS) MRA (3).Methods:
This IRB-approved study was conducted on a 1.5 Tesla scanner (MAGNETOM Avanto, Siemens Healthcare, Erlangen, Germany). A prototype single-shot radial QISS sequence was used for breath-hold and free-breathing acquisitions. Typical imaging parameters included: 97-99 radial views, field of view 260 mm, 3.1-mm slice thickness with 20% slice overlap, 50-60 slices, 3 concatenations for breath-hold acquisitions. Free-breathing acquisitions used navigator gating with a 3-mm navigator window and both leading and trailing navigators. In most subjects, both coronal and axial QISS scans were acquired. Eight subjects were studied including three healthy volunteers and five patients. For the volunteers, the reference standard was CEMRA. In each of the volunteers, at least one Cartesian QISS scan was acquired in addition to radial QISS in order to evaluate the impact of k-space trajectory on image quality. The patients underwent CTA (which served as the reference standard) on the same day as the MR exam in preparation for a pulmonary vein isolation procedure to treat persistent atrial fibrillation. All patients had atrial fibrillation at the time of the MRA study, with RR intervals ranging from ~500 ms to ~1200 ms. Source images and thin multi-planar reconstructions were evaluated by two radiologists, each with more than five years’ experience in the interpretation of pulmonary CTA and body MRA. Twenty-five pulmonary arterial segments were scored for image quality in each subject.Results:
Typical breath-hold times were ~15-20 seconds. Scan times for navigator-gated studies were ~2-3 minutes. Comparing Cartesian and radial QISS MRA, the radial scans consistently showed more uniform intravascular signal intensity and sharper vessel borders. Both breath-hold and navigator-gated single-shot radial QISS MRA provided fair-to-excellent evaluation of pulmonary arterial anatomy (Figure 1). All pulmonary arterial branches down to the segmental level were visualized by breath-hold and navigator-gated QISS. On an individual segmental basis, no significant differences in image quality were found between the breath-hold QISS, navigator-gated QISS and CEMRA protocols by either radiologist reader. Aggregating data across all pulmonary arterial segments, both readers preferred breath-hold QISS to navigator-gated QISS (P<0.05). Reader 1 preferred CEMRA to both breath-hold and navigator-gated QISS (P<0.001), whereas reader 2 preferred breath-hold QISS to CEMRA (P<0.001). Inter-reader agreement was fair (kappa = 0.3) for breath-hold QISS, and moderate (kappa = 0.46) for navigator-gated QISS and CEMRA (kappa = 0.42). In patients using CTA as the reference standard, breath-hold and navigator-gated QISS MRA maintained diagnostic quality despite the irregular cardiac rhythm.Discussion and Conclusion:
In this preliminary study, we found that both breath-hold and free-breathing single-shot radial QISS MRA efficiently demonstrated pulmonary arterial anatomy from the main pulmonary trunk through the level of the segmental branches. Navigator-gated acquisitions tended to show mild blurring compared with breath-hold scans, but maintained diagnostic image quality. The single-shot QISS technique was also noted to be resistant to cardiac arrhythmias that were present in all patients. Further studies will be directed towards technique optimization, as well as to evaluating the accuracy of the radial QISS technique in patients with suspected pulmonary embolism.Acknowledgements
No acknowledgement found.References
1. Stein PD, et al. N Engl J Med. 2006 Jun 1;354(22):2317. 2. Nagle SK, et al. Eur J Radiol. 2016 Mar;85(3):553. 3. Edelman RR, et al. J Cardiovasc Magn Reson 2015 Nov 23;17:101.Figures
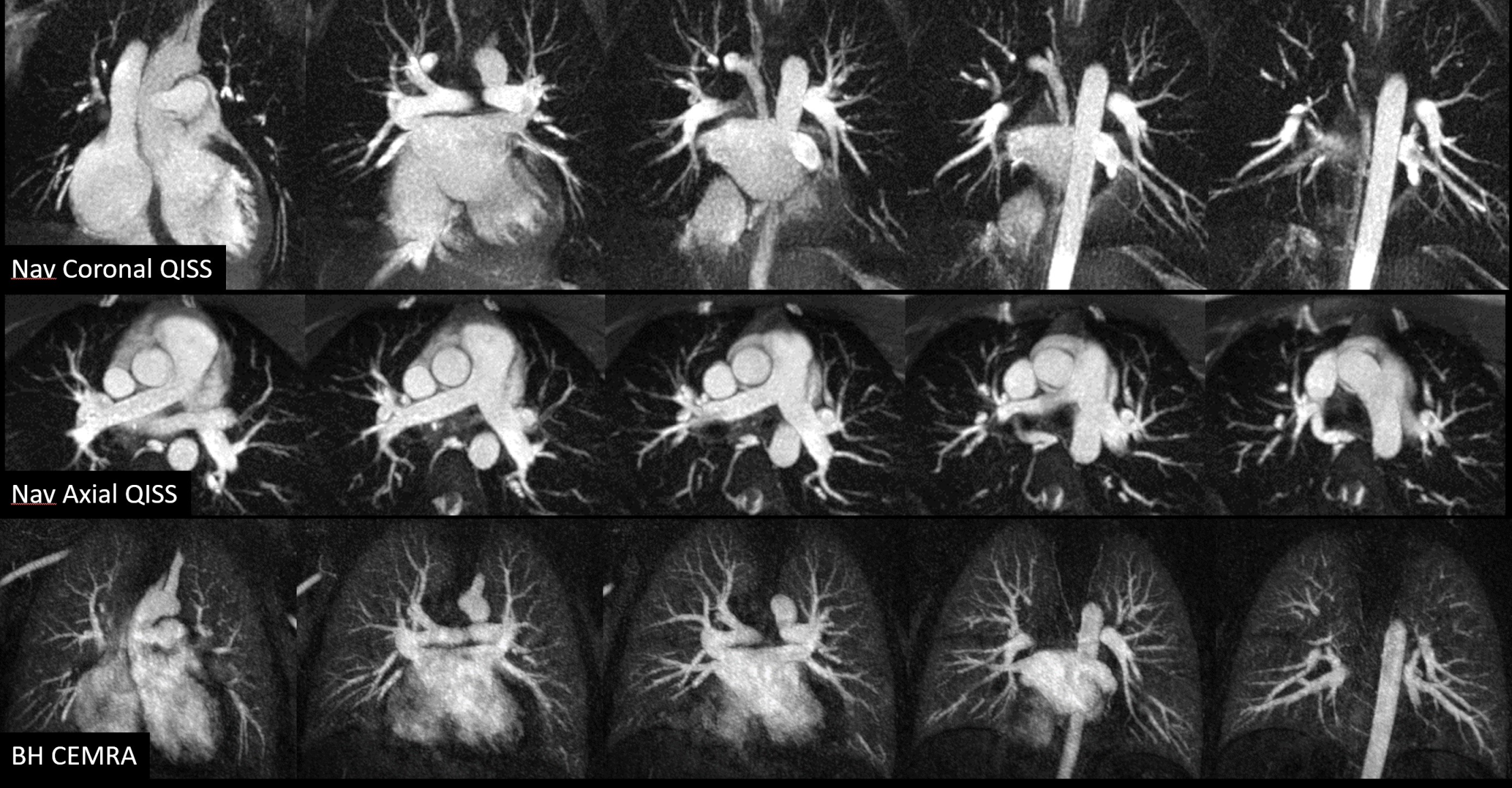
Fig. 1. Comparison of coronal (top row) and axial (middle row) navigator-gated single-shot radial QISS vs breath-hold CEMRA (bottom row). In this subject, the free-breathing QISS MRA provided comparable depiction of the pulmonary arterial anatomy to the CEMRA.