2803
Transluminal Attenuation Gradient in Non-contrast Whole Heart Magnetic Resonance Coronary Angiography (MRA TAG) – Noninvasive Methods for Assessment of Coronary Flow: A Comparison with Coronary Computed Tomography Angiography TAGYuki Ohmoto-Sekine1, Junji Takahashi2, Takashi Yoshida2, Rieko Ishimura3, Makiko Ishihara4, Yasuji Arase1, and Mitsue Miyazaki5
1Health Management Center, Toranomon Hospital, Tokyo, Japan, 2Radiology Dept., Toranomon Hospital, Tokyo, Japan, 3Cardiovascular Center, Toranomon Hospital, Tokyo, Japan, 4Imaging Center, Toranomon Hospital, Tokyo, Japan, 5Toshiba Medical Research Institute, Chicago, IL, United States
Synopsis
CT coronary angiography (CTA) and non-contrast coronary MRA are established non-invasive methods for anatomical assessment of coronary artery stenosis; however, functional information is limited. Transluminal attenuation gradient (TAG) of CTA predicts a functional significant stenosis. The aim of this study was to access TAG using non-contrast whole heart coronary MRA (MRA TAG) as compared to TAG using CTA (CTA TAG). Preliminary evaluation of MRA TAG provides acceptable prediction of invasive FFR. Further study is required to determine an appropriate prediction of MRA TAG.
Purpose
Coronary computed tomography angiography (CTA) and non-contrast whole heart coronary MR angiography (MRA) are established as non-invasive methods for anatomical assessment of coronary artery stenosis; however, functional information is limited. Recently, novel CT technique such as CT derived fractional flow reserve (FFR-CT) and transluminal attenuation gradient (TAG) predicts functional significant stenosis. The aim of this study was to access TAG using MRA (MRA TAG) as compared to TAG using CTA (CTA TAG).Methods
CTA was performed with 80-slice multi-detector-row scanner (Acquilion prime, Toshiba Medical Systems, Otawara, Japan). A biphasic intravenous contrast injection protocol was used that consisted of contrast medium (iopamidol 370mg/ml, Bayer, Germany), depending on the subject’s body weight (22.2mg/kg) followed by mixed normal saline (70%), contrast medium (30%), and 10ml of saline at flow rate, according to the body weight (0.06×body weight ml/s). Non-contrast whole heart coronary MRA was acquired using a 1.5T MRI scanner (Vantage powered by ATLAS, Toshiba Medical Systems, Otawara, Japan). The CTA and MRA data were transferred to a workstation (Zio Workstation, Amin Ltd., Tokyo, Japan) for analysis. The cross-sectional images perpendicular to the vessel centerline were reformatted for each major coronary artery. The luminal radiological contrast attenuation on CTA (Hounsfield units [HU]) and signal values on MRA were measured at 5-mm intervals along the artery from the ostium to the distal level where the cross-sectional area decreased to 2.0 mm2. The contour of the region of interest and the vessel centerline were manually corrected if necessary. CTA TAG was determined from the change in HU per 10- mm length of coronary artery and defined as a linear regression coefficient between intraluminal radiological attenuation (HU) and length from the ostium (mm). MRA TAG was also determined from the change in signal value per 10-mm length of coronary artery. Considering the signal value of MRI is a relative value, we calculated the degree of leaning with the value that was set as the ratio of 1 for the first signal near the ostium at each coronary artery. Thus MRA TAG was defined as a linear regression coefficient between the ratio and length from the ostium (mm). A previously described, the cut off value of CTA TAG was defined - 15.1 HU/ 10 mm predicted FFR _0.8 (1). We analyzed asymptomatic 7 subjects, with suspicious stenotic lesion from the coronary artery MRA screening, underwent to the CT scan. Wilcoxon-t test was used for the visible vessel length. Correlation of CTA TAG and MRA TAG was assessed via linear regression analysis.Results
Seven cases, 21 arteries were evaluated in this study. Visible vessel length of CTA was longer than that of MRA (p = 0.018, Table 1). Of 21 arteries, 3 hypoplastic vessels (3 left circumflex arteries) were excluded. Four vessels were indicated significant stenosis as less than -15 HU/ 10 mm in CTA TAG. A representative case is shown in Figure 1. There was good agreement for both CTA TAG and MRA TAG by the linear regression analysis (y = 0.0032x + 0.0074, r = 0.85, Figure 2). The cut off value -15HU/ 10 mm provided in CTA TAG was thought to be equivalent to the value -0.05/ 10 mm obtained in MRA TAG.Discussion
Preliminary results suggest that noninvasive quantification of MRA TAG was feasible. From the linear progression analysis, there was an excellent correlation between CTA TAG and MRA TAG. The cut off value -15HU/ 10 mm provided in CTA TAG was thought to be equivalent to the value in MRA TAG. As compared to CTA, the visible vessel length of MRA was generally shorter; it may change the cut off value. However, we may be able to assess the appropriate physiological information without an additional scan by depicting a proper length of coronary arteries.Conclusion
Assessment of MRA TAG provides acceptable prediction for invasive FFR and may provide a noninvasive, simple, and easily modality for detecting functional significant coronary stenosis. Further study is required to determine the appropriate prediction of MRA TAG and to understand its potential utility.Acknowledgements
No acknowledgement found.References
1) Wong D.T.L. et al, J of Am Coll Cardiol 61:1271-1279, 2013.Figures
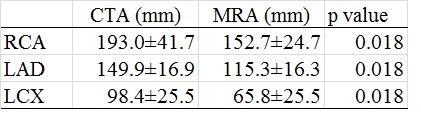
Table 1 Visible vessel length of CTA and MRA

Figure 1. Representative case of CTA and
MRA with TAG.
Right coronary artery with a stenotic
lesion by CTA (A-1) and MRA (B-1). A-2) Blue
dots represent 5-mm intervals at intraluminal attenuation (HU) (A-2) and signal
value (B-2). A-3) Axial and cross
sectional views show CTA (A-3) and MRA (B-3).
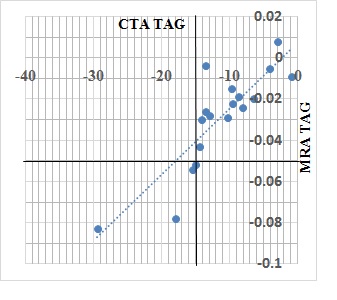
Figure 2.
Correlation of CTA TAG and MRA TAG was assessed via
linear regression analysis. (y = 0.0032x
+ 0.0074, r = 0.85)