2794
Precision and Reproducibility of Cardiac Phase Resolved Ventricular Volumetry using 4D MUSIC MRI in Congenital Heart Disease1Diagnostic Cardiovascular Imaging Laboratory, David Geffen School of Medicien at UCLA, Los Angeles, CA, United States, 2Department of Radiology, David Geffen School of Medicien at UCLA, Los Angeles, CA, United States, 3Department of Medicine, David Geffen School of Medicien at UCLA, Los Angeles, CA, United States
Synopsis
Precise and reproducible quantification of ventricular function and volume, particularly right ventricular volumetry, is important in congenital heart disease. Accurate quantification is highly dependent on accurate delineation of myocardial borders. Ferumoxytol-enhanced MUSIC provides multiphase, high resolution, dynamic 3D imaging of the whole heart. We evaluated the precision and reproducibility of ventricular function and volumetric measurements using a commercial 3D image design and modeling software whose segmentation algorithm takes into account partial volume effects (Mimics, Materialise). We demonstrate that quantification of ventricular function and volumetry for 4D MUSIC images using Mimics is reproducible with high intra-class correlation coefficient.
BACKGROUND
Ferumoxytol (Feraheme, AMAG Pharmaceuticals, Waltham, MA), as an off-label MRI contrast agent, has a long intravascular half-life and high relaxivity1, which enables clear depiction of intra-cardiac and vascular borders. Three-dimensional time-resolved (4D) MUSIC, leverages ferumoxytol to provide higher spatial resolution2 images of the beating heart and related vascular structures. The images can be reformatted in any arbitrary plane following image acquisition, which is valuable in CHD due to frequently complex intra-cardiac anatomy. In addition, reproducible quantification of ventricular volumetry is important, for which MRI remains the gold standard. We aimed to evaluate the precision and intra- observer reliability of semi-automatic biventricular function and volume quantification of 4D MUSIC MRI.METHODS
Twenty-one consecutive patients (12 females, mean age 4± 3 years) with known CHD who underwent ferumoxytol-enhance MUSIC MRI were included. All exams were performed at 3.0T and ferumoxytol up to 4mg/kg were administered. Twelve patients had echocardiographic m-mode derived measures of biventricular volume and ejection fraction (EF). MUSIC MRI DICOM data were reconstructed into three-dimensional model and processed using a commercial software (Mimics V19.0, Materialise, Leuven, Belgium). One observer independently defined end-diastolic (ED) and end-systolic (ES) phase visually using a widely available commercial software (OsiriX®, Geneva, Switzerland). The left ventricular (LV) and right ventricular (RV) endocardial borders were manually contoured (twice, at 1-month interval) to generate EF and biventricular volumes in the ED and ES phase (LVEDV, LVESV, RVEDV, RVESV) and Intra- observer reproducibility of MUSIC volumetry was assessed by using intra-class correlation coefficient (ICC). Bland-Altman plots were generated to evaluate limits of agreement. MUSIC volumetry and functional measurements were compared to LVEDV, LVESV and LVEF derived from echocardiography.RESULTS
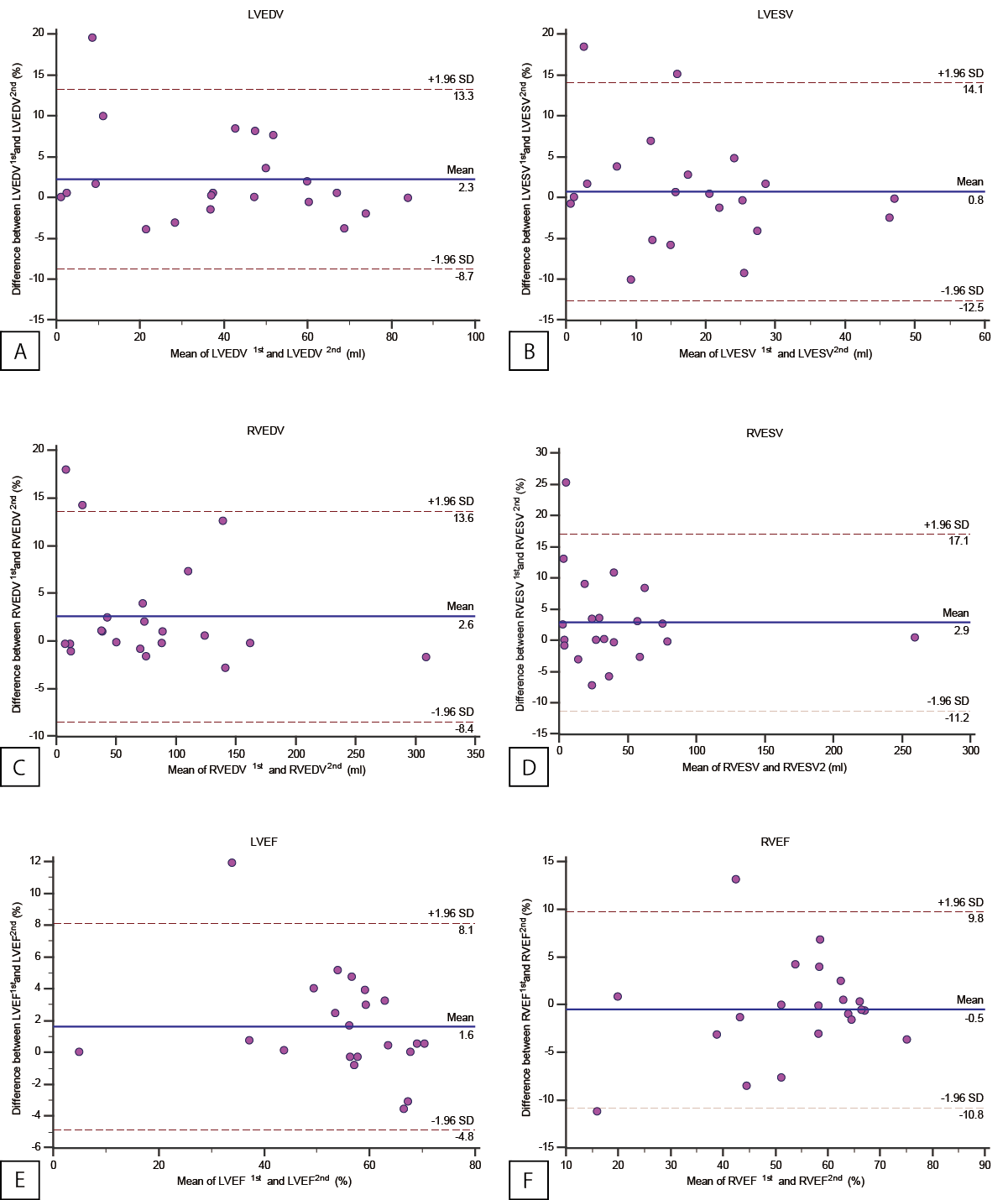
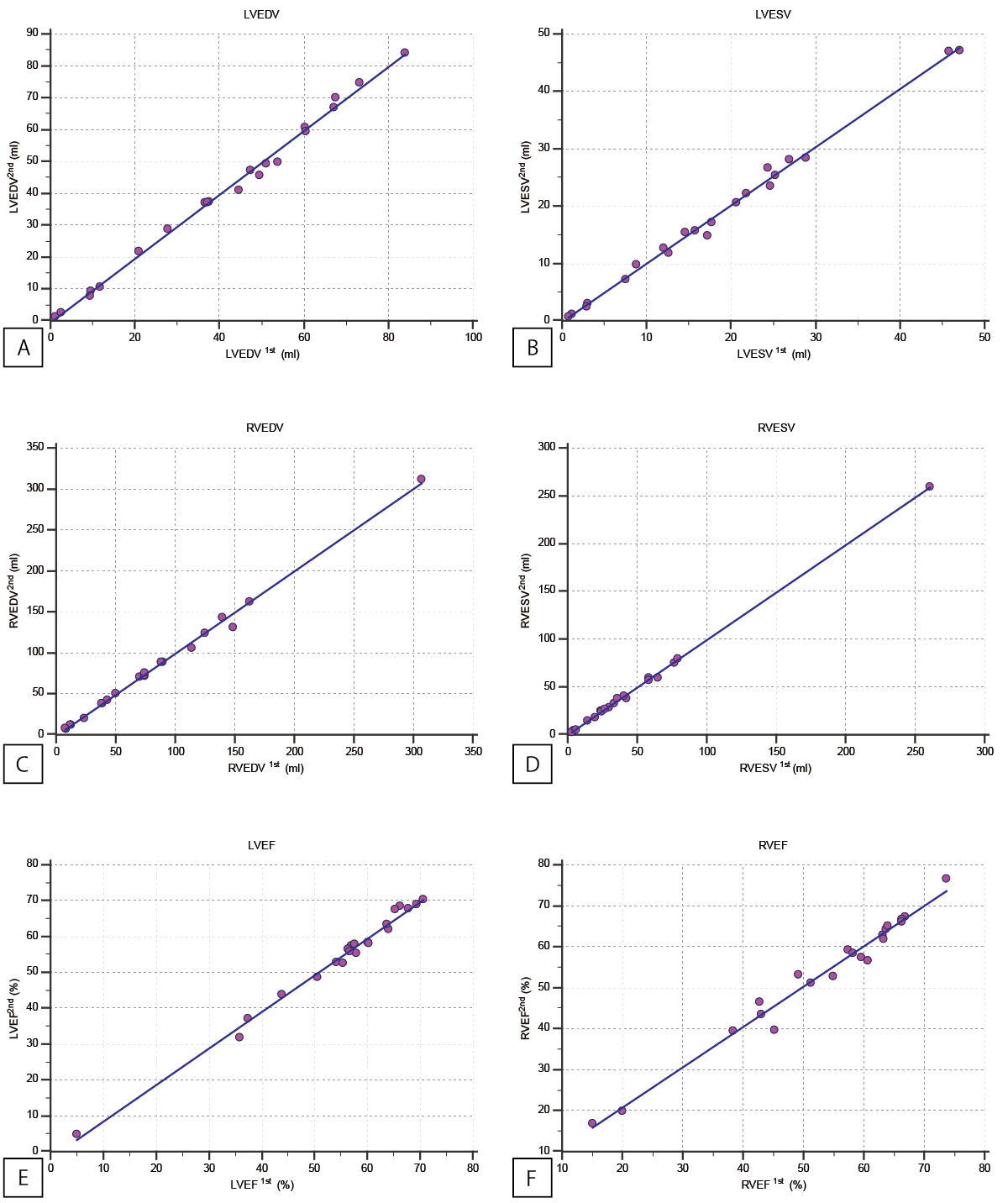
All MUSIC MRI scans were completed successfully and without complications. The predominant diagnoses were variations of Tetralogy of Fallot. Intra- observer reliability for all measurements of biventricular EDVs, ESVs and EFs was excellent (Figure 1): LVEDV (r = 0.998, p<0.0001), LVESV (r = 0.997, p<0.0001), LVEF (r = 0.995, p<0.0001), RVEDV (r = 0.998, p<0.0001), RVESV (r = 1, p<0.0001) and RVEF (r = 0.988, p<0.0001). The Bland-Altman plot also shows acceptable intra-observer reproducibility as reflected in the bias and 95% limits of agreement (LOA): LVEDV (P = 0.08, lower LOA = -8.73 (CI -13.16 to -4.29), upper LOA = 13.26 (8.83 to 19.47)), LVESV (P = 0.60, lower LOA = -12.53 (-17.91 to -7.16), upper LOA = 14.1 (8.73 to 17.7)), LVEF (P = 0.03, lower LOA = -4.84 (-7.45 to -2.23), upper LOA = 8.11 (5.5 – 10.72)), RVEDV (P = 0.05, lower LOA = -8.45 (-12.9 to -3.99), upper LOA = 13.64 (9.18 to 18.09)), RVESV (P = 0.08, lower LOA = -11.18 (-16.88 to -5.48), upper LOA = 17.07 (11.37 to 22.76)), RVEF (P = 0.67, lower LOA = -10.77 (-14.91 to -6.63), upper LOA = 9.77 (5.62 to 13.91)). Volumetry and functional parameters between MUSIC and echocardiography correlated moderately for LVEDV (r = 0.79, p=0.01), LVESV (r = 0.55, p=0.07) and LVEF (r = 0.82, p<0.01).CONCLUSION
Semi-automated quantification of biventricular function and volumetry for MUSIC can be performed with high precision and reproducibility using a commercial 3D modeling software and has implications for accurate and simplified automation of 3D cardiac function and volumetry.Acknowledgements
No acknowledgement found.References
1. Li W, Tutton S, Vu AT, et al. First-pass contrast-enhanced magnetic resonance angiography in humans using ferumoxytol, a novel ultrasmall superparamagnetic iron oxide (USPIO)-based blood pool agent. J Magn Reson Imaging 2005;21:46–52.
2. Han, F., Zhou, Z., Han, E., Gao, Y., Nguyen, K.-L., Finn, J. P. and Hu, P. (2016), Self-gated 4D multiphase, steady-state imaging with contrast enhancement (MUSIC) using rotating cartesian K-space (ROCK): Validation in children with congenital heart disease. Magn. Reson. Med.. doi:10.1002/mrm.26376
Figures