2790
Accelerated multi-contrast high isotropic resolution 3D intracranial vessel wall MRI using a tailored k-space undersampling and partially parallel reconstruction strategy.1University of Washington, Seattle, WA, United States, 2Philips Healthcare, Beijing, People's Republic of China
Synopsis
Identification and differentiation of intracranial vessel wall pathologies requires multi-contrast high isotropic resolution 3D vessel wall MRI. However scan times for multi-contrast intracranial vessel wall imaging (IVWI) are too long to be tolerated by patients. We have developed a tailored k-space undersampling and partially parallel reconstruction strategy to accelerate 0.5mm 3D isotropic multi-contrast IVWI sequences to five minutes each. We demonstrate an accelerated multi-contrast IVWI protocol that provides similar vessel delineation as fully sampled sequences. Protocol performance was assessed in patients with intracranial atherosclerotic disease and showed clear delineation of vessel wall and atherosclerotic plaque.
Introduction
Stroke is a leading cause of death and morbidity worldwide, and intracranial vascular disease is a significant contributor. Intracranial Vessel Wall Imaging (IVWI) has potential to evaluate disease beyond current angiographic methods by directly detecting vessel wall pathology. IVWI requires high isotropic resolution of the order of 0.5mm(1) due to small thin walled vessels and complex vessel geometry. Moreover, lesion differentiation requires a multi-contrast protocol with several sequences. Thus multi-contrast IVWI protocols can have prohibitively long scan times. Previous studies (2-4) have demonstrated 0.5mm isotropic IVWI but are restricted by use of single sequences or long scan times per sequence. A multi-contrast IVWI protocol requires short scan times to be tolerated by debilitated patients and avoid motion artifacts.Aim
To develop a 3D 0.5mm isotropic multi-contrast IVWI with scan time of 5 minutes per sequence while retaining reconstructed spatial resolution similar to fully sampled IVWI.Methods
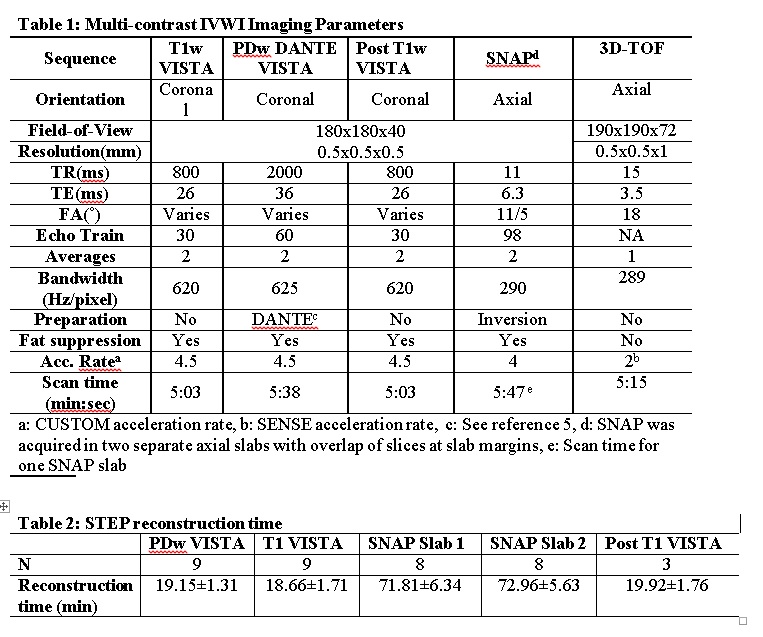
The target multi-contrast VWI sequences were 0.5mm x 0.5mm x 0.5mm resolution (interpolated to 0.25mm x 0.25mm x 0.25mm), Pre-contrast T1w-VISTA, DANTE (5) prepared PDw-VISTA, SNAP(6) and Post-contrast T1w-VISTA. Acceleration by k-space undersampling was achieved using Cartesian Under-Sampling with Target Ordering Method (CUSTOM)(7) and partially-parallel imaging (PPI) reconstruction was performed using Self-supporting Tailored k-Space Estimation for Parallel Imaging Reconstruction (STEP)(8) for VWI sequences only . In addition to VWI sequences, the full protocol acquired 3D-TOF and CE-MRA. Target scan time was 5 minutes per sequence and 30 minutes for the full protocol. Protocol parameters are provided in table 1. All scans were carried out on a Philips Ingenia 3T scanner with 32 channel head coil. Post-contrast T1w-VISTA was scanned 3 minutes after single dose gadolinium contrast injection (0.1 mmol/kg of Prohance at 2cc/sec) in patients with intracranial atherosclerotic disease (ICAD).
K-space undersampling with CUSTOM: For IVWI, an auto-calibration region of size 26x26 voxels was fully sampled. Given an acceleration factor, CUSTOM undersampling pattern was generated point by point using a parametric variable radius sampling scheme. Optimized CUSTOM parameters 𝛽l and 𝛽g that control the width of the local and global sampling distributions were set to 0.22 and 0.33 respectively(7). Acceleration factors of 4.5X was used for PDw-VISTA, pre-contrast T1w-VISTA and post-contrast T1w-VISTA and 4X for SNAP to achieve 5 minute scan time for each sequence.
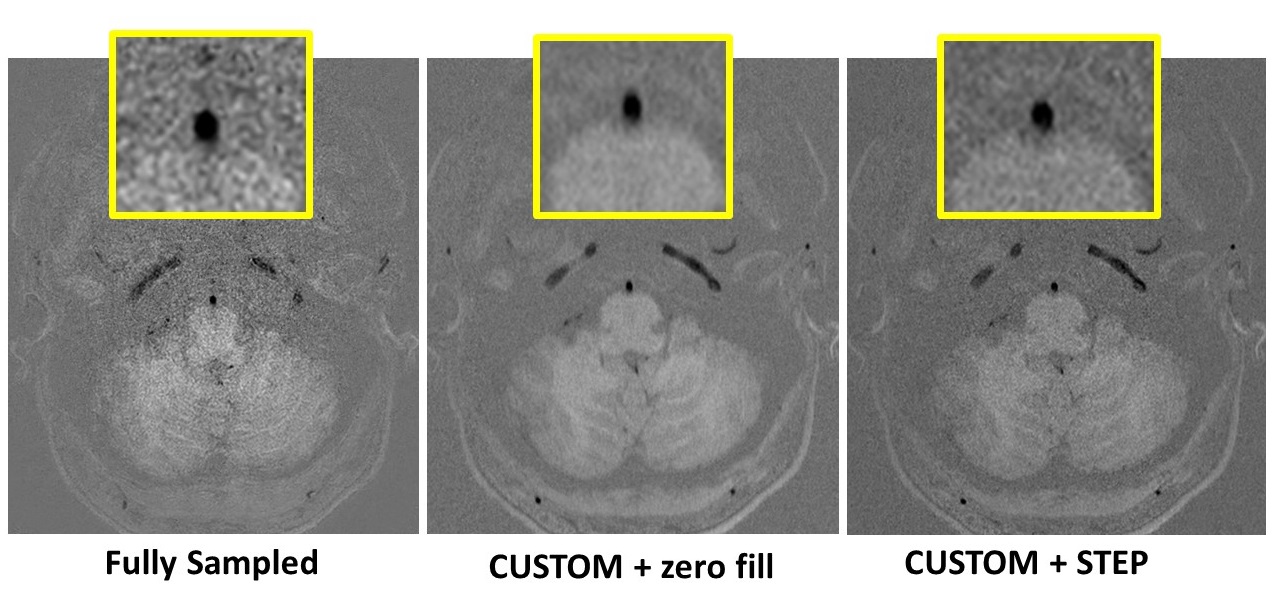
STEP PPI reconstruction: STEP reconstruction was performed offline using Matlab Parallel Processing Toolbox on a workstation with Intel Xeon Processor 2.4 GHZ with eight cores, 32 GB RAM and NVIDIA GeForce GTX TITAN X GPU with 3584 cores. The two images from SNAP (inversion-recovery and reference) were jointly reconstructed and SNAP corrected real images were calculated. Reconstruction times were recorded for each sequence.
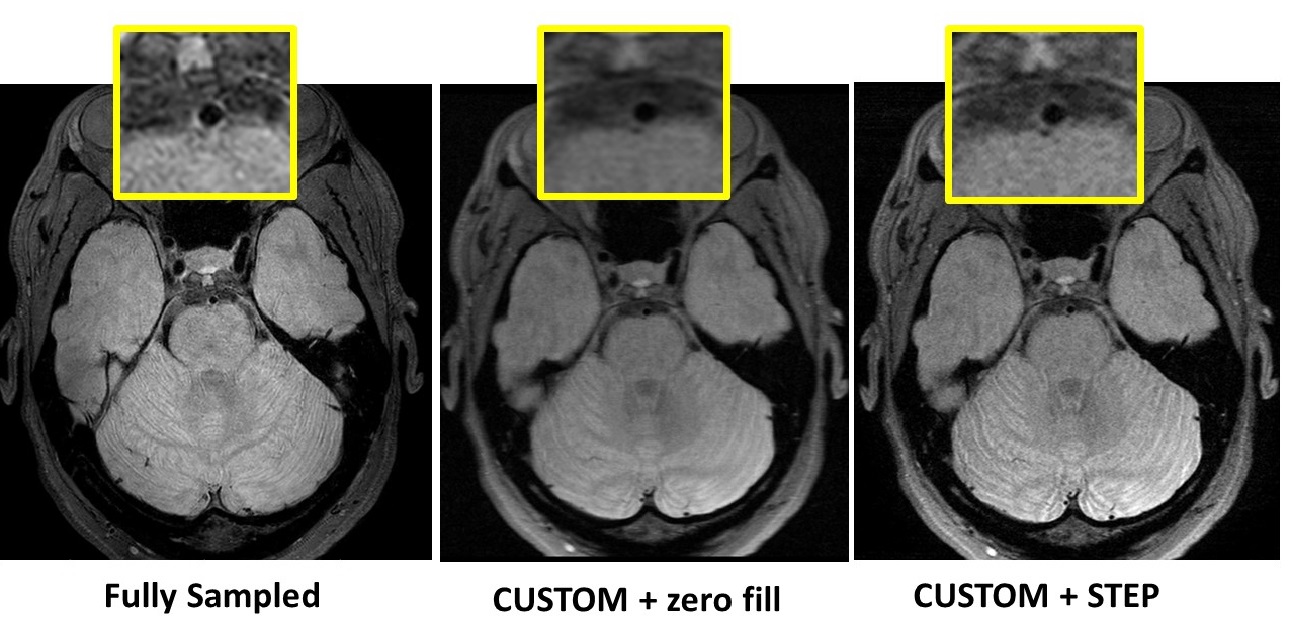
Comparison to full-sample VWI: CUSTOM undersampled and STEP reconstructed scans were compared to full-sample VWI (figures 1 and 2) in one volunteer.
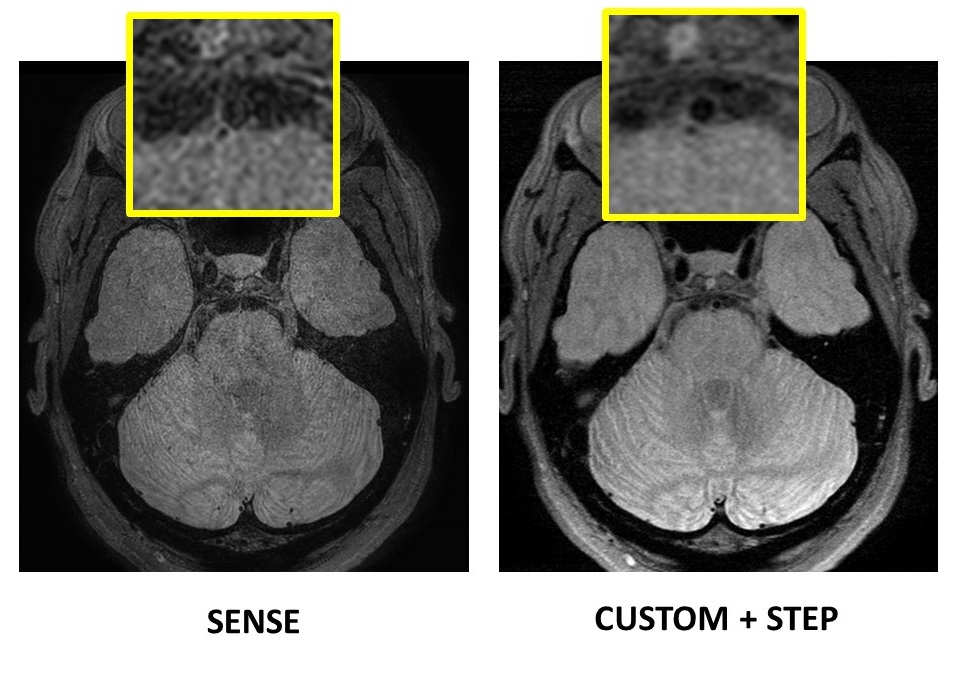
Comparison to SENSE: SENSE accelerated (2.25X) PDw-VISTA was compared to PDw-VISTA CUSTOM+STEP in one volunteer (figure 3). Scan time was similar and other imaging parameters (PDw-VISTA in table 1) were identical between the scans.
Evaluation of protocol performance: The optimized IVWI protocol was tested in 6 volunteers and in 2 patients with known ICAD stenosis by clinical MRA. Patients received gadolinium contrast and post-contrast T1w-VISTA was obtained.
Results
Comparison to full-sample VWI: Scan times for full-sample PDw-VISTA, T1w-VISTA and SNAP were 12:38, 10:04 and 12:24 mins respectively with no averaging. CUSTOM+STEP PDw-VISTA (figure 1) and T1w-VISTA provided comparable vessel wall delineation as full-sample versions. CUSTOM+STEP SNAP showed superior luminal contrast compared to full-sample SNAP (figure 2).
Comparison to SENSE: SENSE acceleration did not provide comparable SNR to CUSTOM+STEP for PDw-VISTA nor provides adequate vessel wall delineation (figure 3). SNAP and T1w-VISTA have lower inherent SNR than PDw-VISTA and are not expected provide adequate vessel delineation with SENSE acceleration.
Evaluation of protocol performance: The full IVWI protocol (total scan time of 35 mins) was well tolerated by patients. Step reconstruction provided improved vessel wall delineation over zero-filled fourier reconstruction (figures 1 and 2). ICAD plaque was clearly visualized in patients (figure 4). PDw-VISTA, T1w-VISTA and post-contrast T1w-VISTA were reconstructed in less than 20 minutes. Joint STEP reconstruction of SNAP required about 70 minutes per volume (table 2 shows average reconstruction times).
Conclusions
CUSTOM+STEP acceleration allowed multi-contrast 3D 0.5mm isotropic VWI within 35 minutes. CUSTOM+STEP provided improved vessel wall delineation than full-sample IVWI when considering all contrast weightings. CUSTOM+STEP is superior to SENSE for IVWI. The full protocol was well tolerated by patients and shows good delineation of ICAD plaque.Acknowledgements
Funding provided by NIH R01NS092207References
1. Qiao Y, Steinman DA, Qin Q, et al. Intracranial arterial wall imaging using three-dimensional high isotropic resolution black blood MRI at 3.0 Tesla. J Magn Reson Imaging. 2011;34(1):22-30.
2. Dieleman N, Yang W, van der Kolk AG, et al. Qualitative Evaluation of a High-Resolution 3D Multi-Sequence Intracranial Vessel Wall Protocol at 3 Tesla MRI. PLoS One. 2016;11(8):e0160781.
3. Fan Z, Yang Q, Deng Z, et al. Whole-brain intracranial vessel wall imaging at 3 Tesla using cerebrospinal fluid-attenuated T1-weighted 3D turbo spin echo. Magn Reson Med. 2016.
4. Zhang L, Zhang N, Wu J, Huang Y, Liu X, Chung YC. High resolution three dimensional intracranial arterial wall imaging at 3 T using T1 weighted SPACE. Magn Reson Imaging. 2015;33(9):1026-34.
5. Li L, Miller KL, Jezzard P. DANTE-prepared pulse trains: a novel approach to motion-sensitized and motion-suppressed quantitative magnetic resonance imaging. Magn Reson Med. 2012;68(5):1423-38.
6. Wang J, Bornert P, Zhao H, et al. Simultaneous noncontrast angiography and intraplaque hemorrhage (SNAP) imaging for carotid atherosclerotic disease evaluation. Magn Reson Med. 2012;69:337-45.
7. Zhou Z, Chen S, Sun A, Li Y, Li R, Yuan C. Optimized Parametric Variable Radius Sampling Scheme for 3D Cartesian k-Space Undersampling Pattern Design. ISMRM2016.
8. Zhou Z, Wang J, Balu N, Li R, Yuan C. STEP: Self-supporting tailored k-space estimation for parallel imaging reconstruction. Magn Reson Med. 2015.
Figures