2785
Identification of Carotid Lipid-Rich Necrotic Core by Three-Dimensional Magnetization-Prepared Rapid Acquisition Gradient-Echo Imaging1Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University, Beijing, People's Republic of China, 2Department of Radiology, University of Washington, Seattle, WA, 3Department of Radiology, Peking University First Hospital, Beijing, People's Republic of China, 4Department of Radiology, Uppsala University Hospital, Sweden
Synopsis
Carotid atherosclerotic lipid-rich necrotic core (LRNC) is associated with ischemic cerebrovascular events. Currently, LRNC was mainly characterized by contrast-enhanced T1 weighted (CE-T1W) or T2 weighted (T2W) imaging. However, CE-T1W imaging needs gadolinium application and T2W imaging is challenging to identify LRNCs with long-T2 components. This study investigated the usefulness of MP-RAGE in identifying carotid LRNC by comparing with CE-T1W and T2W imaging. We found that LRNC had the lowest relative signal intensity against muscle or fibrous tissue on MP-RAGE images among three sequences (P<0.05), indicating that MP-RAGE might be a better non-contrast imaging tool to identify LRNC than T2W imaging.
Introduction
It has been demonstrated that characteristics of lipid-rich necrotic core (LRNC), one of the key features of atherosclerotic vulnerable plaques, are significantly associated with ischemic cerebrovascular events1. Previous studies reported that LRNC can be identified using T2-weighted (T2W) or contrast-enhanced T1-weighted (CE-T1W) imaging sequence after combining with T1W imaging and time-of-flight (TOF) MR angiography2-4. A study by Cai et al has shown that the CE-T1W imaging was better than T2W imaging in quantification of LRNC validated by histology3. However, CE-T1W imaging might not be applicable for patients with renal dysfunction. Therefore, it is suggested to propose a non-contrast imaging approach that has a better performance than T2W imaging in characterizing LRNC.
Histologically, LRNC is usually composted of cholesterol crystal, debris of apoptotic cells, particles of calcium, etc. Previous study showed that the T1 value of LRNC and fibrous tissue in the vessel wall was 519 ms and 596 ms, respectively5. As such, it is challenging to distinguish LRNC from fibrous tissue using traditional T1W imaging. It is well established that heavily T1 weighted imaging displays better contrast than traditional T1W imaging, particularly for tissues with small differences in T1 values6. Three-dimensional magnetization-prepared rapid acquisition gradient-echo (MPRAGE), as a heavily T1-weighted sequence, has been largely used to delineate white/gray matter of brain7. We hypothesized that MPRAGE might be capable of identifying LRNC in carotid atherosclerotic plaque.
Purpose
To investigate the usefulness of three-dimensional MPRAGE in identifying carotid LRNC.Methods
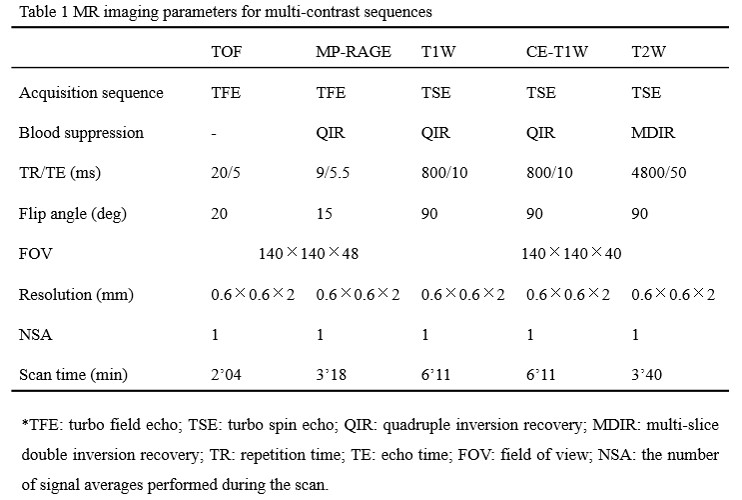
A total of 12 patients were randomly selected from a study which recruited symptomatic patients with carotid plaques on ultrasound. MR imaging: All subjects underwent carotid multicontrast MR vessel wall imaging on a 3.0T MR scanner with dedicated 4-channel carotid coil. The MR imaging protocol included TOF, T1W, T2W, CE-T1W, MP-RAGE imaging sequences. The imaging parameters are detailed in Table 1. Image review: Two reviewers interpreted the MR images with consensus. The contours for lumen, outer wall, region of interest (ROI) in the sterno-cleidomastoid muscle and plaque components including LRNC and calcification (CA) at each axial location were outlined according to the published criteria8. Specifically, the LRNC was mainly identified by CE-T1W images at each axial location. The signal intensity (SI) was measured for the fibrous tissue (FT), LRNC, calcification, and muscle on the images of each imaging sequence. The relative SI (rSI) of plaque components, including LRNC and CA, against muscle or FT was calculated according to the minimum SI of plaque components versus the mean SI of muscle or FT. The rSI of plaque components against muscle or FT was compared among CE-T1W, T2W, and MP-RAGE sequences. The slices with intraplaque hemorrhage in carotid arteries were excluded.Results
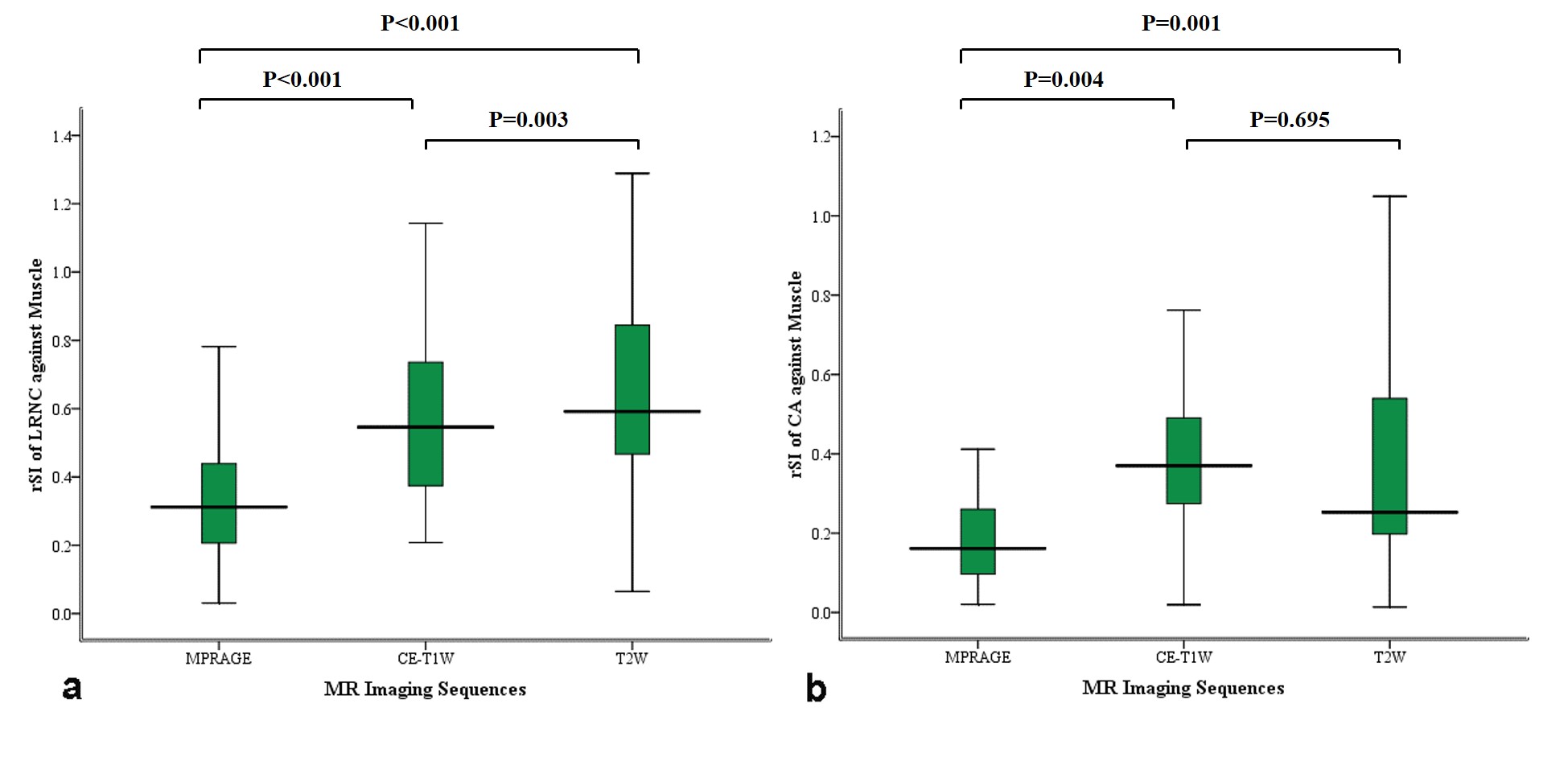
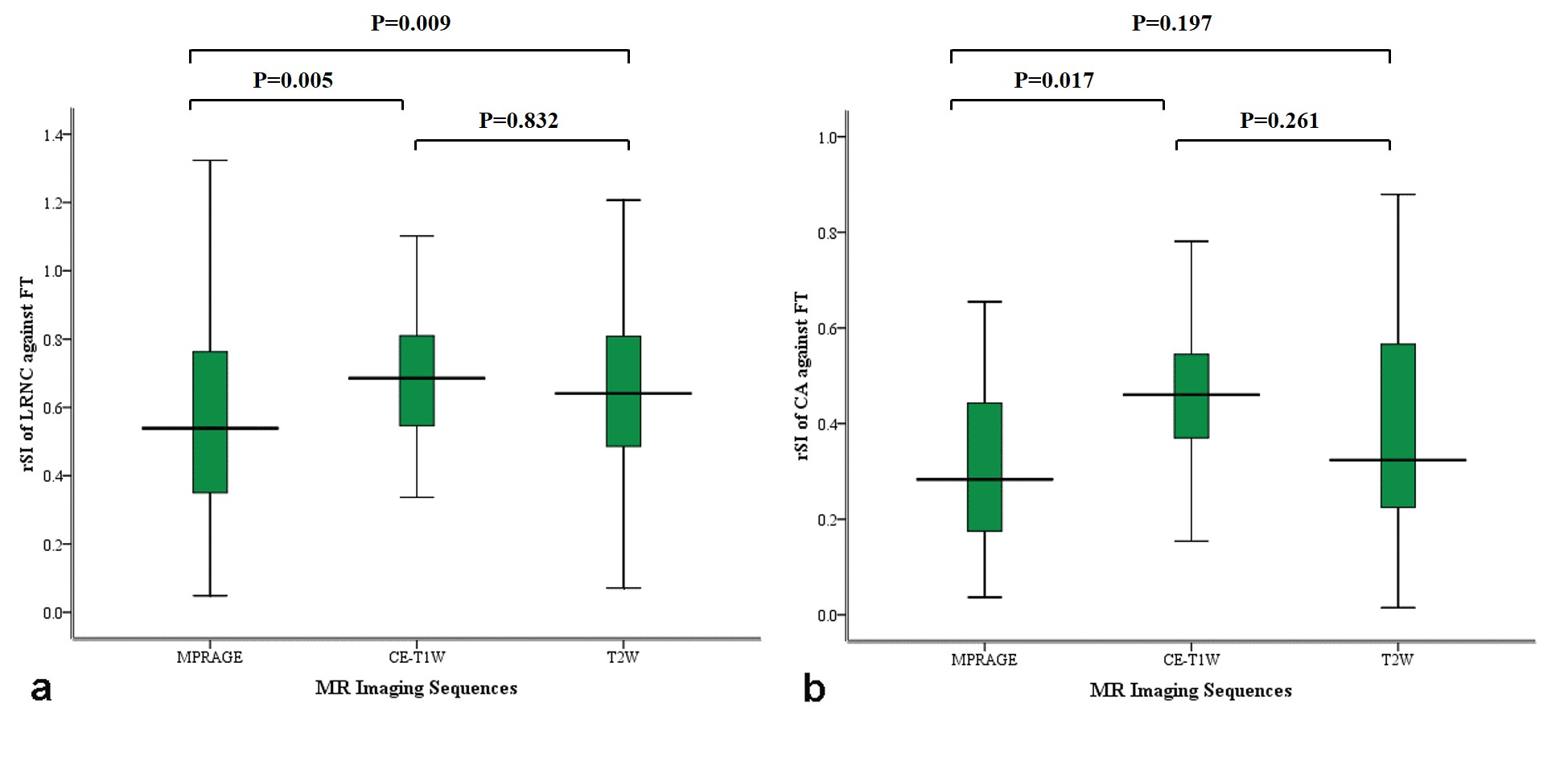
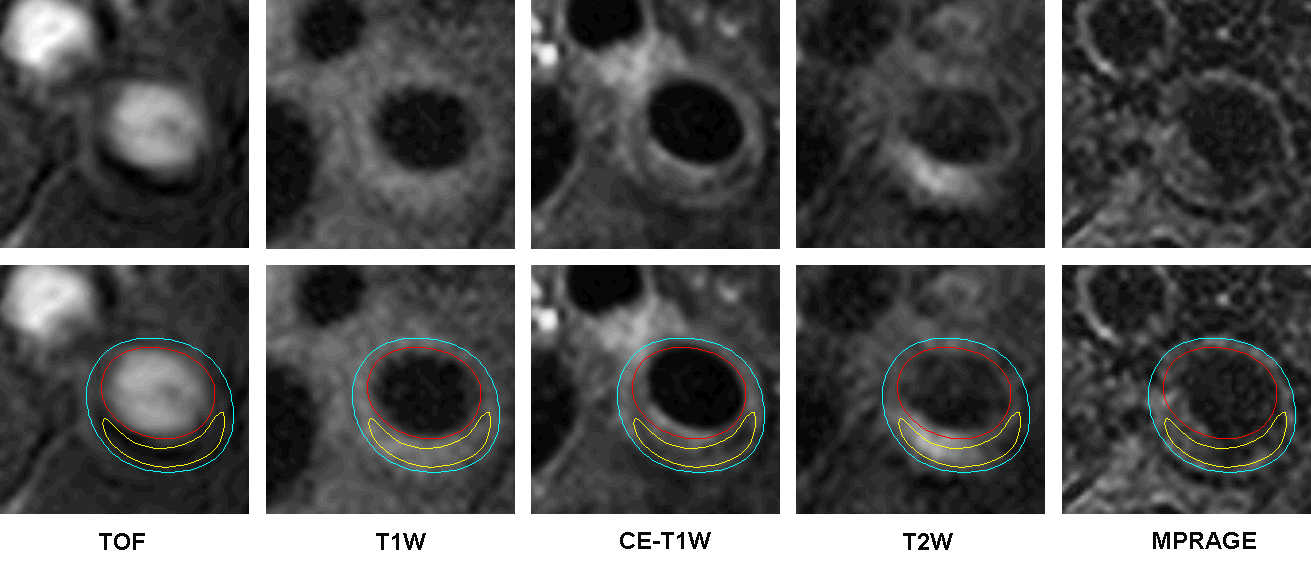
In total, 11 subjects with 21 arteries and 352 slices with acceptable image quality were eligible for image review. Of 352 slices, 88 (25.0%) slices had LRNC, and 31 (8.8%) slices had CA. The rSIs of LRNC against muscle in different sequences were summarized in Figure 1a. The MP-RAGE images showed the lowest rSI of LRNC against muscle (0.34±0.18), followed by CE-T1W (rSI: 0.58±0.23) and T2W (rSI: 0.71±0.47) images. Similarly, the MP-RAGE images showed the lowest rSI of LRNC against FT (0.57±0.26), followed by T2W images (0.67 ±0.27), and CE-T1W (0.68±0.19). The rSIs of CA among different sequences were summarized in Figure 1b. The MP-RAGE images showed the lowest rSI of CA against muscle (0.20±0.16), followed by CE-T1W (0.40±0.21) and T2W (0.43±0.40) images. In contrast, the rSI of CA against FT was 0.33±0.23, 0.46±0.18, and 0.40 ±0.23 on MPRAGE, CE-T1W, and T2W images, respectively. The rSIs of LRNC and CA against FT in different sequences were summarized in Figure 2. Figure 3 was an example that MP-RAGE successfully delineated LRNC. The region of LRNC showed lower SI than muscle on CE-T1W and MPRAGE images but appeared high SI on T2W images.Discussion
In this study, we investigated the usefulness of three-dimensional MP-RAGE in identifying carotid LRNC by comparing with CE-T1W and T2W imaging. Both LRNC and CA had the lowest rSIs against muscle or FT on MP-RAGE images compared with CE-T1W and T2W imaging. There was a substantial overlap of rSIs between LRNC and CA, whereas CA shows lower SI than LRNC on TOF and T1W images3,9. Our findings suggest that it is feasible to identify LRNC by using MP-RAGE sequence combined with TOF and T1W imaging. Investigation of the performance of MP-RAGE in identifying LRNC is warranted in future studies with larger sample size and histology validation.Conclusion
The MP-RAGE sequence might be a better non-contrast imaging tool to identify carotid LRNC than T2W imaging.Acknowledgements
None.References
1. Zavodni AE, Wasserman BA, McClelland RL, et al. Carotid artery plaque morphology and composition in relation to incident cardiovascular events: the Multi-Ethnic Study of Atherosclerosis (MESA). Radiology. 2014;271(2):381-389.
2. Trivedi RA, U-King-Im JM, Graves MJ, et al. MRI-derived measurements of fibrous-cap and lipid-core thickness: the potential for identifying vulnerable carotid plaques in vivo. Neuroradiology. 2004;46(9):738–743.
3. Cai J, Hatsukami TS, Ferguson MS, et al. In vivo quantitative measurement of intact fibrous cap and lipid-rich necrotic core size in atherosclerotic carotid plaque: comparison of high-resolution, contrast-enhanced magnetic resonance imaging and histology. Circulation. 2005;112(22):3437-3444.
4. Takaya N, Cai J, Ferguson MS, et al. Intra- and interreader reproducibility of magnetic resonance imaging for quantifying the lipid-rich necrotic core is improved with gadolinium contrast enhancement. J Magn Reson Imaging. 2006;24(1):203-210.
5. Jiang Y, Zhu C, Peng W, et al. Ex-vivo imaging and plaque type classification of intracranial atherosclerotic plaque using high resolution MRI. Atherosclerosis. 2016;249:10-16.
6. Mugler JP 3rd, Brookeman JR. Three-dimensional magnetization-prepared rapid gradient-echo imaging (3D MP RAGE). Magn Reson Med. 1990;15(1):152-157.
7. Ota H, Yarnykh VL, Ferguson MS, et al. Carotid intraplaque hemorrhage imaging at 3.0-T MR imaging: comparison of the diagnostic performance of three T1-weighted sequences. Radiology. 2010;254(2):551-563.
8. Cai JM, Hatsukami TS, Ferguson MS, et al. Classification of human carotid atherosclerotic lesions with in vivo multicontrast magnetic resonance imaging. Circulation. 2002;106:1368-1373.
9. Yoshida K, Narumi O, Chin M, et al. Characterization of carotid atherosclerosis and detection of soft plaque with use of black-blood MR imaging. AJNR Am J Neuroradiol. 2008;29(5):868-874.
Figures