2777
Motion Insensitive 3D Multiple Echo Inversion Recovery Stack of Star(ME IR SOS) technique for measurement of T2* in Intraplaque Hemorrhage(IPH)1UCAIR, Department of Radiology and Imaging Sciences, University of Utah, Salt Lake City, UT, United States, 2Siemens Healthcare, 3Department of Veterans Affairs, VASLCHCS
Synopsis
The purpose of this work was to develop a 3D ME IR SOS technique to reduce off resonance blurring and allow measurement of T2* in Atherosclerotic plaque. In a prior study we observed lower ADC values in symptomatic IPH. We hypothesized that the T2* measurements from 3D ME IR SOS would help identify IPH and further characterize symptomatic and asymptomatic IPH. The 3D ME IR SOS can provide motion insensitive IPH visualization and T2* values simultaneously which may provide important clinical information to detect the plaque progression.
PURPOSE
Intraplaque hemorrhage (IPH) detected with carotid MRI identifies plaques at increased risk of future and recurrent stroke.1-3 Our prior research has shown that the 3D Inversion Recovery Stack of Star (IR SOS) sequence consistently improved carotid IPH images by decreasing artifact due to motion and incomplete blood flow suppression.4 The purpose of this work was to develop a 3D Multiple Echo (ME) IR SOS technique to reduce off resonance blurring and allow measurement of T2* in atherosclerotic plaque. In a prior study we observed lower ADC values in symptomatic IPH.5 We hypothesized that T2* measurements from 3D ME IR SOS would help identify IPH and further characterize symptomatic and asymptomatic IPH.
METHODS
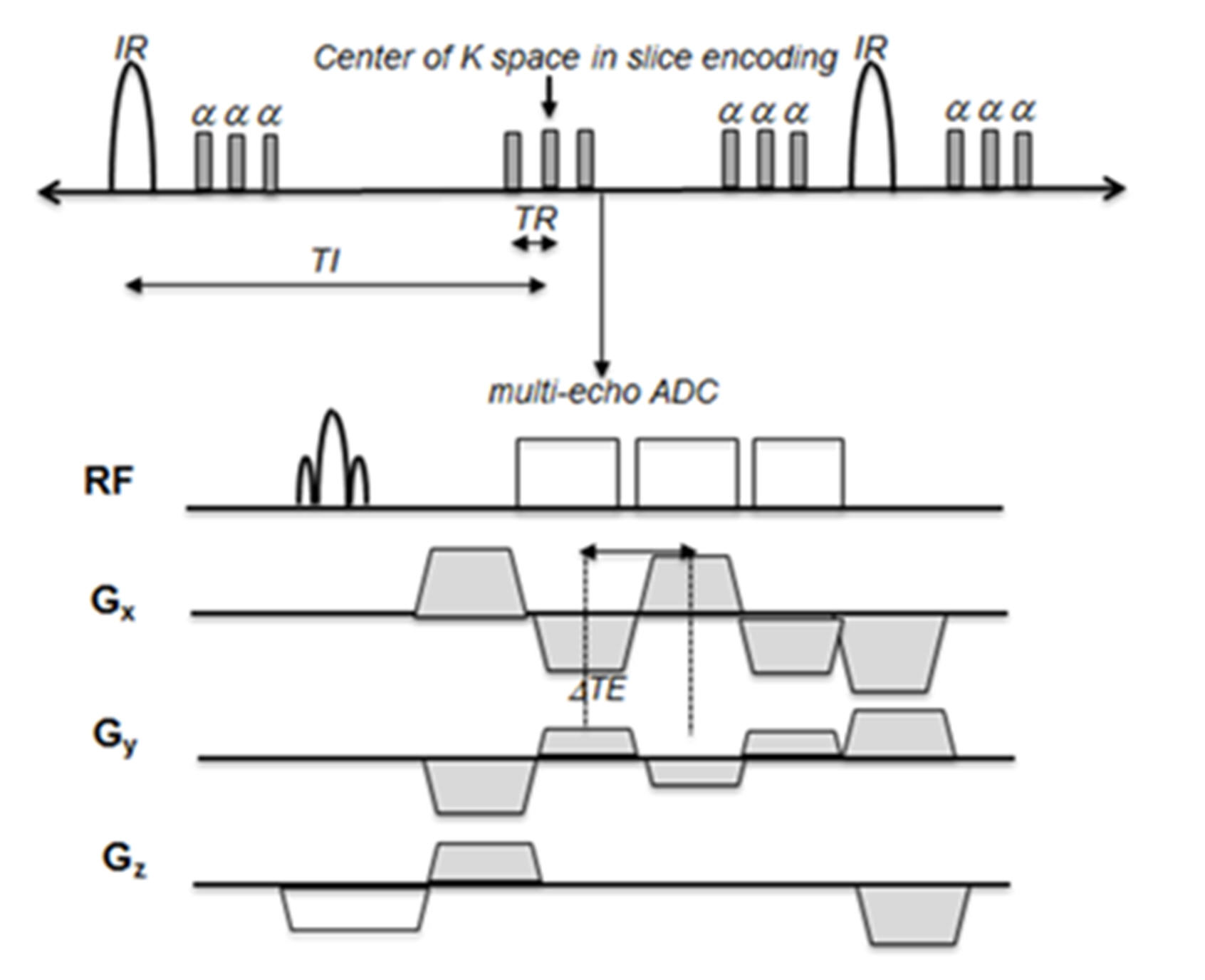
The 3D ME IR SOS sequence was implemented with an inversion recovery (IR) preparation and spoiled segmented fast low angle shot (FLASH) readout.4 IR prep was performed with a nonselective hyperbolic secant adiabatic inversion RF pulse to provide a uniform inversion of spins. After each IR preparation, a series of multiple echo FLASH measurement were acquired for all kz phase encodings in a single SOS view angle. After the inversion time (TI), all phase-encoding steps along the slice direction (“partitions”) are acquired sequentially before lines at different view angles (spokes) are acquired. In each readout, three echoes were acquired. Fig 1 demonstrates the pulse sequence of 3D ME IR SOS. The T2* was calculated with least-square estimation based on the semi-log linear regression of the signal values from all echoes and their corresponding echo time according to the following linear relationship: $$$\frac{\text{}1}{\text{}T2*}=\frac{\text{}lnS_{l}-lnS_{m}}{\text{}TE_{m}-TE_{l}}$$$ where $$$S_{l}$$$ and $$$S_{m}$$$ are signal intensity at the echo time $$$TE_{l} $$$and $$$TE_{m}$$$, respectively. To test the feasibility of the proposed technique, MRI studies of five symptomatic and five asymptomatic patients with with known carotid IPH were performed on a Siemens Trio 3T MRI scanner with home built phased array carotid coils.6 The imaging parameters for 3D ME IR SOS were: coronal plane, FOV=160x160mm2, voxel dimension=0.73mm3, TE1/TE2/TE3/TR = 2.05/4.15/6.25/9.0ms, bandwidths=560hz/pixel, 64slices/slab, TI =350mm. The total imaging time was 3 min 20 sec. 3D T1w SPACE with DANTE preparation measurements were acquired before and after contrast administration. We measured ADC using 3D DWDE SOS sequence.5 T2* and ADC maps were calculated and displayed using IDL. Three ROIs per each patient were selected in IPH for T2* and ADC measurement.RESULTS
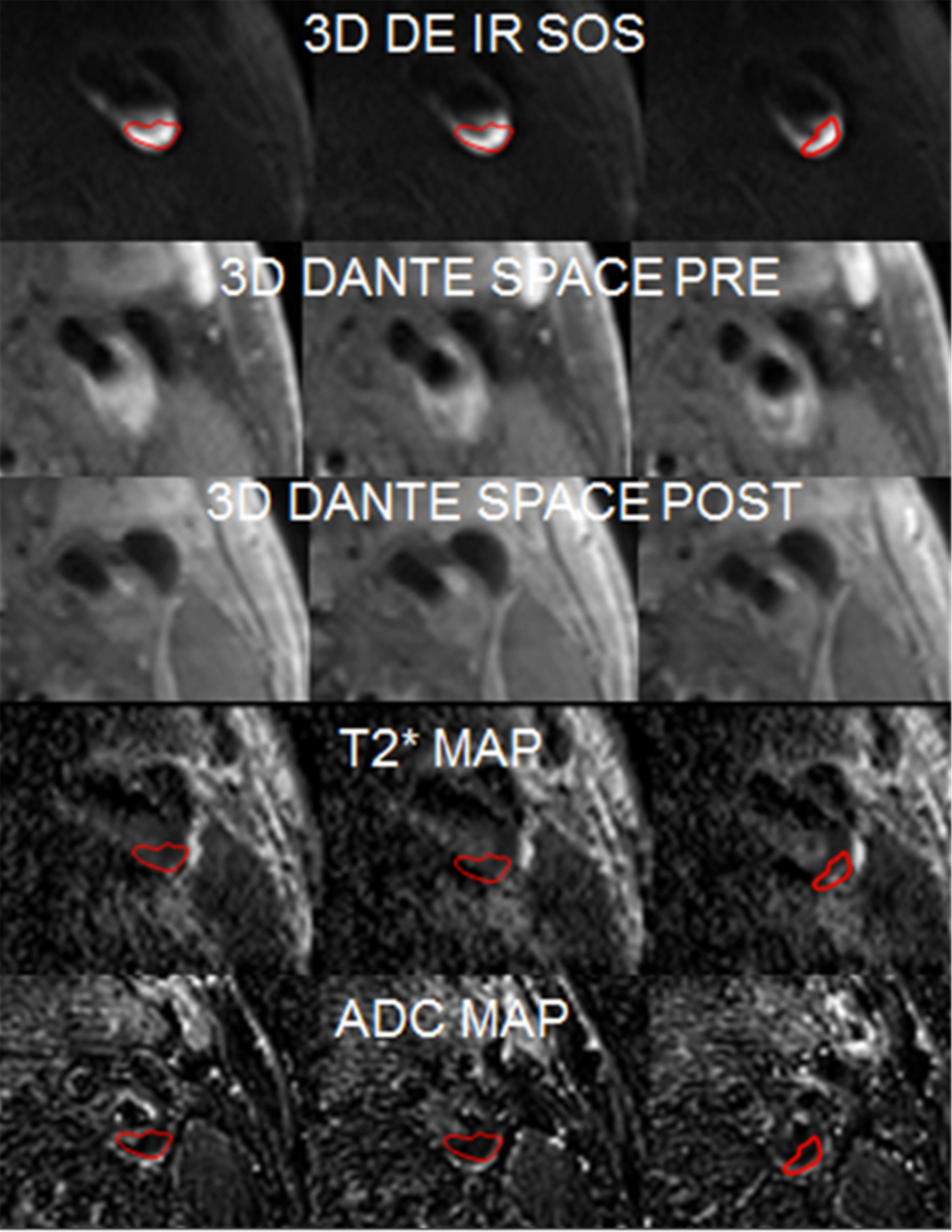
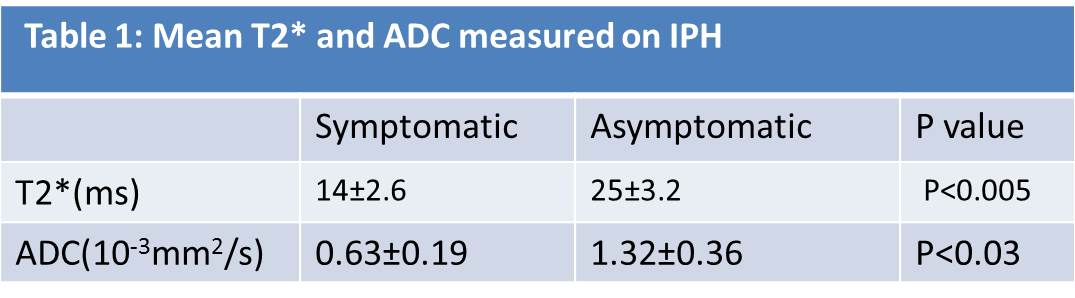
The mean T2* and ADC for IPH obtained from 10 subjects are summarized in Table 1. Symptomatic compared to asymptomatic had significantly lower plaque T2* values (14±2.6 vs. 25±3.2ms, respectively, p<0.005). This value is close to the T2* value reported previously.6,7 Fig 2 displays 3D ME IR SOS, 3D T1w SPACE, T2* and ADC maps from a symptomatic subject with IPH. The ROI drawn by the red lines in the maps Fig 2 demonstrate a typical ROI selection. T2* and ADC values were 15±1.6ms and 0.91±0.17x10-3mm2/s, mean±SD.DISCUSSION
3D ME IR SOS could detect and characterize carotid IPH in atherosclerotic plaque. In symptomatic IPH, T2*-shortening suggests an equilibrium shift of intraplaque iron complexes. Given the greater local effects on magnetic susceptibility, our finding suggests that aggregate iron complexes preferentially form in symptomatic plaque. Further study is needed to determine the amount, species, and chemistry of intraplaque iron complexes and their relationship with the T2* signal change in IPH development and maintenance. The SOS sequence is less sensitive to motion artifacts due to the repeated high-density sampling of the k-space center but is more sensitive to off-resonance effects. The off-resonance sensitivity can be reduced by increased sampling bandwidth. This paper presented triple echo measurements with moderately increased bandwidth. Acquiring more than three echoes with higher bandwidth may allow gradient timing calibration and multi-point fat-water separation in addition to T2* determination.CONCLUSION
3D ME IR SOS can provide motion insensitive IPH detection and T2* map simultaneously which may provide important clinical information to detect vulnerable plaque progression.Acknowledgements
Supported by R01 HL127582, RSNA Research Scholar Grant RSCH1414, Siemens Medical Solutions, the Clinical Merit Review Grant from the Veterans Administration health Care System.References
1. Saam T, Hatsukami TS, Takaya N, et al. The vulnerable, or high-risk, atherosclerotic plaque: noninvasive MR imaging for characterization and assessment. Radiology 2007;244(1):64-77.
2. Gupta A, Baradaran H, Schweitzer AD, et al. Carotid Plaque MRI and Stroke Risk A Systematic Review and Meta-analysis. Stroke 2013;44(11):3071-3077.
3. Moody AR, Murphy RE, Morgan PS, et al. Characterization of complicated carotid plaque with magnetic resonance direct thrombus imaging in patients with cerebral ischemia. Circulation 2003;107(24):3047-3052.
4. Kim SE, Roberts JA, Eisenmenger LB, et al. Motion-insensitive carotid intraplaque hemorrhage imaging using 3D inversion recovery preparation stack of stars (IR-prep SOS) technique. J Magn Reson Imaging. 2016 Jul 7. doi: 10.1002/jmri.25365. [Epub ahead of print]
5. Kim SE, McNally JS, Treiman GS, et al. Motion Insensitive high resolution in vivo DWI of Carotid Artery Wall Imaging using 3D Diffusion Weighted Driven Equilibrium Stack of Stars (3D DW-DE SOS) sequence, Proceedings of the 24th ISMRM, Singapore, 2016
6. Beck MJ, Parker DL, Bolster BD, et al. Interchangeable Receive-Only Carotid Coils for Simultaneous Imaging with Radio Frequency Head Coils at 3 Tesla. Proceedings of the 24th ISMRM, Singapore, 2016
7. Zhu DC, Vu AT, Ota H, et al. An Optimized 3D Spoiled Gradient Recalled Echo Pulse Sequence for Hemorrhage Assessment Using Inversion Recovery and Multiple Echoes (3D SHINE) for Carotid Plaque Imaging. Magn Reson Med. 2010 64:1341–1351
8. Raman SV, Winner MW, 3rd, Tran T, et al. In vivo atherosclerotic plaque characterization using magnetic susceptibility distinguishes symptom-producing plaques. JACC Cardiovasc Imaging 2008;1(1):49-57; PMCID: 2729432.
Figures