2768
Identification of Intrapalque Hemorrhage in Carotid Artery by Simultaneous Non-contrast Angiography and intraPlaque hemorrhage (SNAP) Imaging: A Comparison Study with MP-RAGE1Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University, Beijing, People's Republic of China, 2Beijing Institute for Brain Disorders, Beijing, People's Republic of China, 3Department of Radiology, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People's Republic of China, 4Department of Radiology, University of Washington, Seattle, WA, United States
Synopsis
It is important to accurately identify carotid artery intraplaque hemorrhage (IPH) due to its significant association with ischemic stroke. MP-RAGE sequence has been demonstrated to be the best approach to detect carotid IPH. Recently, investigators proposed SNAP imaging technique which allows non-contrast MR angiography and identifying IPH simultaneously. This study sought to investigate the performance of SNAP imaging in detecting carotid IPH by comparing with MP-RAGE. We found that SNAP imaging detected more IPHs and showed larger IPH size than MP-RAGE, suggesting SNAP imaging might be a sensitive imaging tool to detect IPH.
Introduction
It has been shown that carotid artery atherosclerotic intraplaque hemorrhage (IPH), as one of the key vulnerable features, can accelerate plaque progression and predict ischemic cerebrovascular events [1]. In addition, investigators found that, for patients with carotid plaques with IPH, stenting therapy group developed more new ipsilateral silent ischemic lesions than carotid endarterectomy (CEA) group, suggesting CEA might be a better treatment for carotid plaques with IPH [2]. Therefore, it is important to accurately identify IPH for stroke prevention. Ota et al demonstrated that magnetization-prepared rapid acquisition gradient-echo (MP-RAGE) sequence showed better agreement with histology in identification of carotid artery IPH compared with time-of-flight (TOF) and T1-weighted (T1w) MR imaging [3]. Recently, Wang et al proposed Simultaneous Non-contrast Angiography and intraPlaque hemorrhage (SNAP) imaging sequence which allows non-contrast MR angiography and identification of IPH simultaneously [4]. However, the usefulness of SNAP imaging in assessing carotid IPH is unknown.Purpose
This study sought to investigate the performance of SNAP imaging in characterizing carotid IPH by comparing with MP-RAGE.Methods
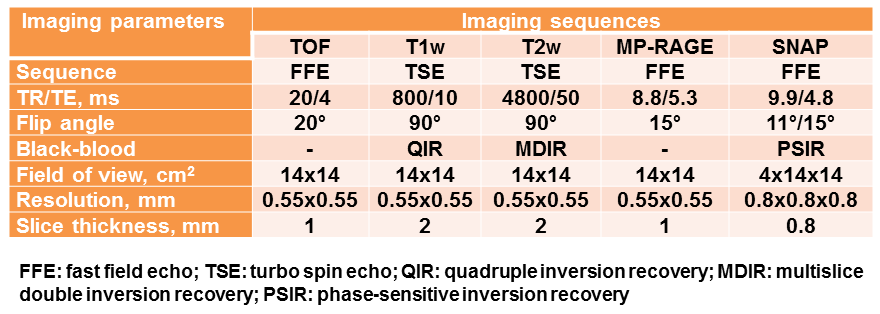
Study sample: Patients with recent cerebrovascular symptoms and carotid atherosclerotic disease (>30% stenosis) were recruited and underwent carotid MR imaging. MR imaging: Carotid MR imaging was performed on a 3.0T MR scanner (Philips, Achieva TX) with 8-channel carotid coil. The MR Imaging protocol included TOF, T1w, T2-weighted (T2w), MP-RAGE, and SNAP sequences. The imaging parameters are detailed in Figure 1. Image review: Two experienced radiologists interpreted the MR images using CASCADE software with consensus. The SNAP images were resliced to cross-sectional images with slice thickness of 2mm. The image review was conducted with two rounds: first round: the reviewers outlined the lumen and outer wall boundaries using all imaging sequences by matching the carotid bifurcation; second round: reviewers detected IPH on MP-RAGE images and SNAP images with lumen and outer wall boundaries separately after one month time interval to minimize memory bias. The IPH on MP-RAGE and SNAP images was defined as hyperintense compared to muscle (signal intensity ratio=1.5:1). Statistical analysis: The agreement between SNAP and MP-RAGE in identifying IPH was determined using Cohen’s Kappa analysis. The volume of IPH on MP-RAGE and SNAP images was compared using paired t test. The study protocol was approved by institutional review board and consent form was obtained from all subjects.Results
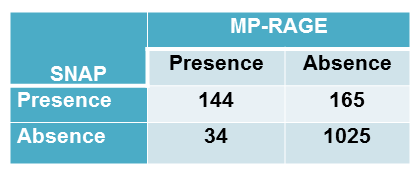
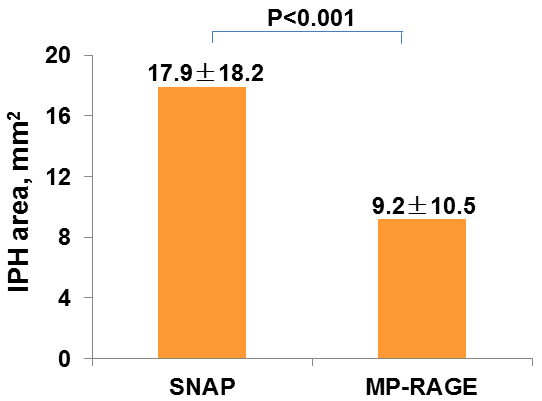
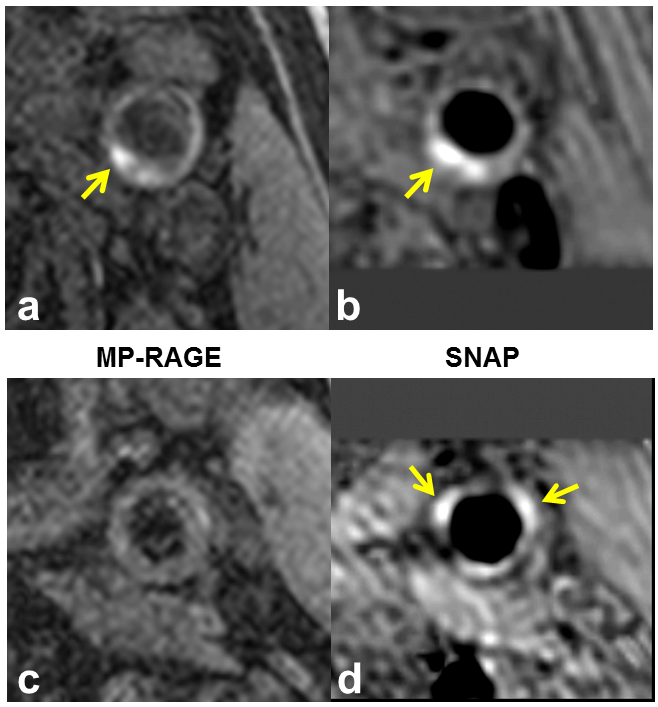
In total, 54 subjects (mean age: 63.1 ± 5.7 years, 38 males) with 108 arteries and 1368 slices having acceptable image quality were included and eligible for image review. Of 108 arteries, 44 (40.7%) and 62 (54.7%) arteries were found have IPH on MP-RAGE and SNAP images, respectively. Of 1368 slices, 178 (13%) and 309 (22.6%) were found to have IPH on MP-RAGE and SNAP images, respectively. Moderate agreement was found between MP-RAGE and SNAP in identification of IPH (k=0.511, P=0.029, Figure 2). For all slices having IPH on both SNAP and MP-RAGE images (n=144), the area of IPH on SNAP was significantly larger than that on MP-RAGE (17.9±18.2 mm2 vs. 9.2±10.5 mm2, P<0.001, Figure 3). Figure 4 represents examples showing IPH on both MP-RAGE and SNAP images with different size (a and b) and IPH was detected by SNAP imaging but not visible on MP-RAGE image (c and d).Discussion
In this study, we investigated the performance of SNAP imaging in identifying carotid IPH and found a moderate agreement between SNAP and MP-RAGE. The SNAP imaging seemed to be more sensitive for IPH and detected more IPHs than MP-RAGE. In addition, the size of IPH was found to be nearly two times larger on SNAP imaging compared with MP-RAGE. This might be due to the larger dynamic range and higher IPH-wall contrast-to-noise ratio of SNAP compared with MP-RAGE [4]. Future studies with larger sample size and histology validation are warranted to further investigate the effectiveness of SNAP imaging in characterizing carotid IPH.Conclusion
The SNAP imaging shows moderate agreement with MP-RAGE in identification of carotid IPH. SNAP imaging detects significantly more IPHs and shows larger IPH size than MP-RAGE, suggesting SNAP imaging might be more sensitive for assessing IPH.Acknowledgements
None.References
1. Saam T, Hetterich H, Hoffmann V, et al. Meta-analysis and systematic review of the predictive value of carotid plaque hemorrhage on cerebrovascular events by magnetic resonance imaging. J Am Coll Cardiol. 2013;62:1081-91.
2. Yamada K, Yoshimura S, Kawasaki M, et al. Embolic complications after carotid artery stenting or carotid endarterectomy are associated with tissue characteristics of carotid plaques evaluated by magnetic resonance imaging. Atherosclerosis. 2011;215:399-404.
3. Ota H, Yarnykh VL, Ferguson MS, et al. Carotid intraplaque hemorrhage imaging at 3.0-T MR imaging: comparison of the diagnostic performance of three T1-weighted sequences. Radiology. 2010;254:551-63.
4. Wang J, Börnert P, Zhao H, et al. Simultaneous noncontrast angiography and intraplaque hemorrhage (SNAP) imaging for carotid atherosclerotic disease evaluation. Magn Reson Med. 2013;69:337-45.
Figures