2767
Cardiac T1 Mapping Using True Hybrid Inversion and Saturation Recovery1GE Healthcare, Bethesda, MD, United States, 2GE Global Research, Munich, Germany, 3GE Healthcare, Waukesha, WI, United States, 4GE Healthcare, Menlo Park, CA, United States
Synopsis
Despite limited accuracy, MOLLI remains popular for T1 mapping due to high precision and visual quality of the maps. This is due primarily to the large dynamic range afforded by the inversion-recovery (IR) acquisition. Methods using saturation-recovery (SR) have better T1 accuracy but have relatively poor precision compared with MOLLI. This work presents a true hybrid IR/SR acquisition that targets the optimal regions of both the IR and SR relaxation curves, employs a novel method for maximizing dynamic range, and uses an improved sampling strategy. The proposed hybrid method combines the accuracy of single-point SR with the precision of IR.
Background
The goal of T1 mapping is to measure tissue T1 with the
highest accuracy and precision possible. Despite systematic underestimation of
T1 and dependence on T2, heart rate (HR), and other imaging parameters resulting
from the Look-Locker readout, MOLLI (1) remains popular owing to its high
precision and visual quality of T1 maps. This is due primarily to the large
dynamic range afforded by the inversion-recovery (IR) acquisition. Single-point
approaches, such as SASHA, SAPPHIRE, and SMART1Map (2-4), achieve T1 accuracy by
using parameter-independent acquisitions. However, precision has been
relatively poor for these methods, especially those using saturation recovery (SR),
compared with MOLLI. This is attributable to the limited range of saturation
delay times (TS), limited number of TSs, and reduced dynamic range. In this
work, we propose a new method for cardiac T1 mapping that uses a true hybrid
IR/SR acquisition designed to combine the
accuracy of single-point SR with the precision of IR. The proposed hybrid
technique uses repeated data
point sampling (5,6) and employs novel means
to maximize the dynamic range and to selectively sample the high-signal regions
of the IR and SR relaxation curves.Methods
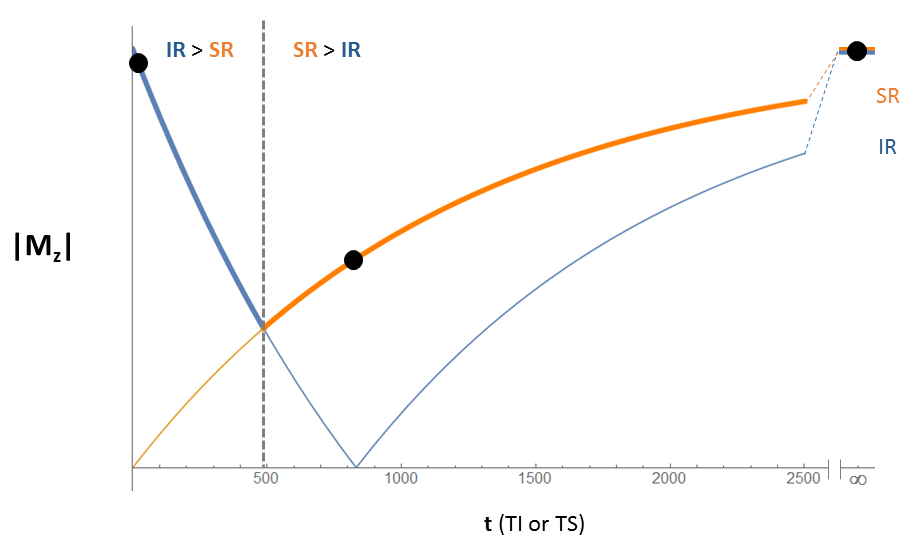
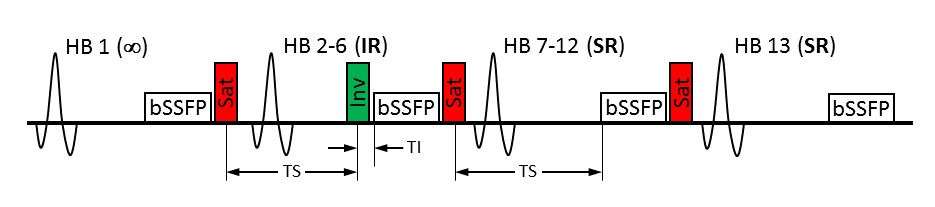
The hybrid acquisition takes advantage of the fact that the IR and SR curves have different relative magnitudes during the recovery process. Data points are acquired only on the thick curve in Figure 1, using IR when the IR curve has higher signal and using SR when the SR curve has higher signal. The hybrid IR/SR pulse sequence is shown in Figure 2 and requires 13 heartbeats. The first heartbeat is used to acquire data at an “infinite” delay time. The next five heartbeats repeatedly sample a data point on the IR curve. To maximize the dynamic range for IR, the longest possible TS and shortest inversion time (TI) are used. Unlike other SR methods, where the maximum intra-heartbeat TS is limited by the trigger delay (TD), a longer TS is achieved here by placing the saturation pulse immediately after the preceding readout. The final seven heartbeats repeatedly sample a data point on the SR curve. To generate T1 maps, data is simultaneously fit to two equations, depending on the acquisition:
$$$A-Be^{-(\frac{TS}{T1})}$$$ for SR and $$$A-2Be^{-(\frac{TI}{T1})}+Ae^{-(\frac{TS+TI}{T1})}$$$ for IR (7).
Because TS is heart-rate dependent, all heartbeats are measured to ensure accurate TS values. Monte Carlo simulations of a native myocardial scan at 1.5T with a constant HR of 60 bpm were performed to compare the precision of the hybrid sequence to that of SASHA, SAPPHIRE, SMART1Map, and MOLLI. Phantom experiments on a 1.5T system were conducted to validate the simulations (T1=1200ms, TR/TE=2.8/1.2ms, FA=65°, TD=674ms, readout=168ms). To assess HR sensitivity, the hybrid sequence was also evaluated with HR that varied arbitrarily throughout the scan (range: 41-86 bpm). Each phantom scan was performed 10 times. Volunteer scans were also performed with both MOLLI and the hybrid sequence.
Results
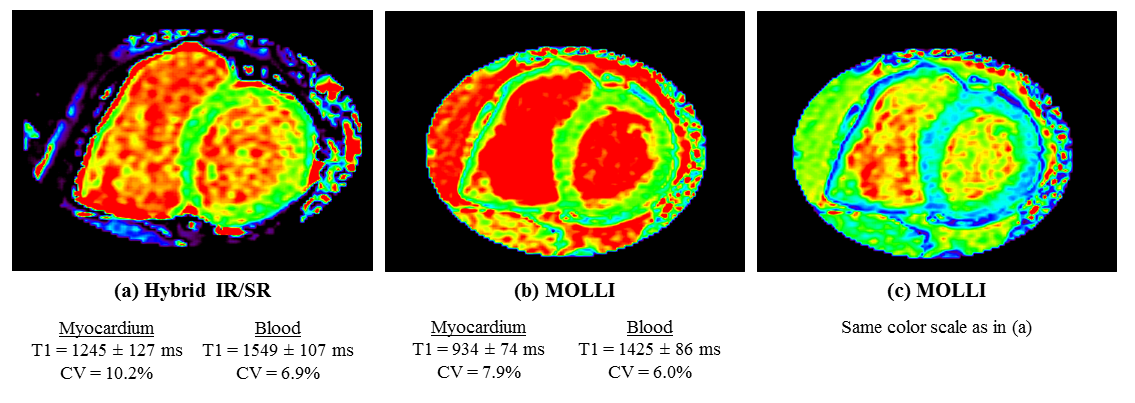
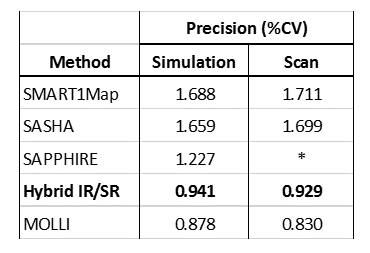
The simulation and scan results are shown in Table 1. In the simulations, SASHA and SMART1Map had the lowest precision, with SAPPHIRE higher by approximately 25%. The hybrid IR/SR method should provide an additional 25% improvement in precision over SAPPHIRE. Phantom scans showed very good agreement with the simulations. The hybrid sequence acquired with variable HR (CV=0.978%) did not result in any loss of precision versus constant HR (CV=1.009%). Volunteer images are shown in Figure 3. MOLLI has higher precision, whereas hybrid IR/SR has higher accuracy. The T1 inaccuracy of MOLLI results in a greater difference between measured blood and myocardial T1, leading to the improved appearance in Figure 3b.Discussion
The results demonstrate that the hybrid method has the best
combination of accuracy and precision compared with existing breath-held T1
mapping techniques. Although SAPPHIRE also uses both inversion and saturation
pulses, the proposed method is expected to outperform SAPPHIRE due to a longer
TS for greater dynamic range, true hybrid IR/SR sampling for maximizing SNR,
and improved sampling point selection. Additionally, unlike other methods, the
maximum TS of the hybrid sequence is independent of TD because the saturation
pulse is decoupled from the ECG trigger; precision is therefore maintained even
for systolic imaging. Precision is also expected to be tolerant of HR
variation. In fact, long arrhythmias can improve precision. While MOLLI still has somewhat better
precision than the hybrid approach, MOLLI cannot provide the accuracy and
objectivity of true T1 measurements typical of single-point acquisitions. Although
the repeated sampling point strategy used in this work was validated for SR
acquisitions, further investigation is required to determine the optimal
strategy for the hybrid acquisition.Acknowledgements
No acknowledgement found.References
1. Messroghli DR et al. Modified Look-Locker Inversion Recovery (MOLLI) for High-Resolution T1 Mapping of the Heart. Magn Reson Med 2004; 52:141-146
2. Chow K et al. Saturation Recovery Single-Shot Acquisition (SASHA) for Myocardial T1 Mapping. Magn Reson Med 2014;71:2082-2095
3. Weingartner S et al. Combined Saturation/Inversion Recovery Sequences for Improved Evaluation of Scar and Diffuse Fibrosis in Patients with Arrhythmia or Heart Rate Variability. Magn Reson Med 2014; 71:1024-1034
4. Slavin GS et al. Breath-Held Myocardial T1 Mapping Using Multiple Single-Point Saturation Recovery. Proc Intl Soc Mag. Reson Med 2012; 20:1244
5. Kellman P et al. Optimized saturation recovery protocols for T1-mapping in the heart: influence of sampling strategies on precision. J Cardiovasc Magn Reson 2014; 16:55
6. Akçakaya M et al. On the Selection of Sampling Points for Myocardial T1 Mapping. Magn Reson Med 2014; 73:1741-1753
7. Deichmann R et al. Optimisation of the 3D MDEFT sequence for anatomical brain imaging: technical implications at 1.5 and 3T. NeuroImage 2004; 21:757-767
Figures