2758
Coronary artery disease is not related to pathologic epicardial fat volumes, left ventricular strain or T1-relaxation times in hypertensive patients1Radiology, University Hospital Bonn, Bonn, Germany, 2Philips Healthcare, Hamburg, Germany
Synopsis
Hypertension is related to increased amounts of epicardial fat, to myocardial fibrosis and to left-ventricular contractility disturbances despite a normal systolic left-ventricular ejection fraction. However, the presence of stable coronary atherosclerotic disease in general - and with no cardiac damage due to prior coronary pathologies - does not additionally affect these parameters.
Introduction
Hypertension has been related to increased amounts of epicardial fat, to myocardial fibrosis and to an impaired left ventricular (LV) contractility 1-5. However, the relationship with a stable coronary atherosclerosis disease (CAD) in general - when no cardiac damage due to prior coronary pathologies occurred - is controversial 1-2, 5-8. Cardiac magnetic resonance (CMR) allows for an accurate volumetric quantification of epicardial fat, for quantification of myocardial tissue changes by T1-mapping to detect myocardial fibrosis as well as for the assessment of LV strain to detect subtle contractility disturbances using dedicated feature tracking softwares 9-11. In this study CMR was used to assess epicardial fat volume (EFV), T1-relaxation time (T1) and LV strain in hypertensive patients with no history of cardiovascular events or cardiac damage. Results werre correlated with the presence of CAD.Materials and Methods
98 hypertensive patients (58 men; 63±11years[y]; BMI 29±6kg/m²) and 25 gender, age and BMI matched controls without CV risk factors or disease were examined at 1.5 Tesla. No patient had a history of cardiac damage due to prior coronary events. EFV normalized to the body surface area [ml/m²] was assessed by a 3D transversal ECG- and respiratory navigator gated magnetization prepared mDixon-sequence. A 3(3)3(3)5 modified Look-Locker inversion recovery (MOLLI) scheme was used to assess T1 [ms]. Myocardial strain [in %] was evaluated by longitudinal strain measurement (LS) in 4-chambre long axis view cine datasets, and circumferential strain measurement (CS) in short axis view cine datasets, using a dedicated feature tracking software (2D Cardiac Performance Analysis MR, TomTec, Unterschleissheim, Germany). All statistical analyses were performed in SPSS, (IBM SPSS Statistics 22.0, Armonk, New York).Results
Hypertensive patients had significantly higher EFV and T1 and lower CS&LS than the non-hypertensive controls (p<0.05); this was independent of the presence of CAD
- controls (n=25): EFV 58±21, T1 967±17, LS -25±5, CS -29±5
- hypertensive patients overall (n=98): EFV 71±25, T1 991±46, LS: -21±4, CS: -25±6
- hypertensive patients without CAD (n=56): EFV 71±27, T1 992±48, LS -21±5, CS -25±6
- hypertensive patients with CAD (n=42): EFV 71±24, T1 987±39, LS -21±4, CS -26±5
No significant differences were found between hypertensive patients with and without CAD. There were also no significant differences between hypertensive patients with CAD when grouped according to the number of vessels affected (0-, 1-, 2- or 3-vessel disease).
Discussion
Hypertension is related to signs of myocardial fibrosis and to LV contractility disturbances, presumably due to hypertension associated cardiac remodeling 5. Hypertension is also related to an increased epicardial fat volume which also may promote the development of myocardial fibrosis as well as an impaired LV contractility through metabolically and inflammatory mechanisms. However, CAD - in the absence of previous coronary events and myocardial damage - did not additionally affect these parameters in the present study. Such a relationship would rather relate to the presence of previous acute pathophysiology with consecutive myocardial damage than to coronary atherosclerosis in general.Acknowledgements
No acknowledgement found.References
[1] Tanami et al. Circ Cardiovasc Imaging 2015;8(3):e002676. [2] Ngo et al. Circ Cardiovasc Imaging 2015;8(3). [3] Yi et al. J Cardiovasc Magn Reson 2015;17:15. [4] Ambale Venkatesh et al. Hypertension 2014;64(3):508-15. [5] Donekal et al.Circ Cardiovasc Imaging 2014;7(2):292-302. [6] Crendal et al. BMC Cardiovasc Disord 2014;14:95. [7] Kim et al. Circ J 2015;79(4):818-24. [8] Yanez-Rivera et al. Cardiovasc Ultrasound 2014;12:35. [9] Hor et al. JACC Cardiovascular imaging 2010;3(2):144-51. [10] Homsi et al. Int J Cardiovasc Imaging 2015. [11] Liu et al. Journal of the American College of Cardiology 2013;62(14):1280-7.
Figures
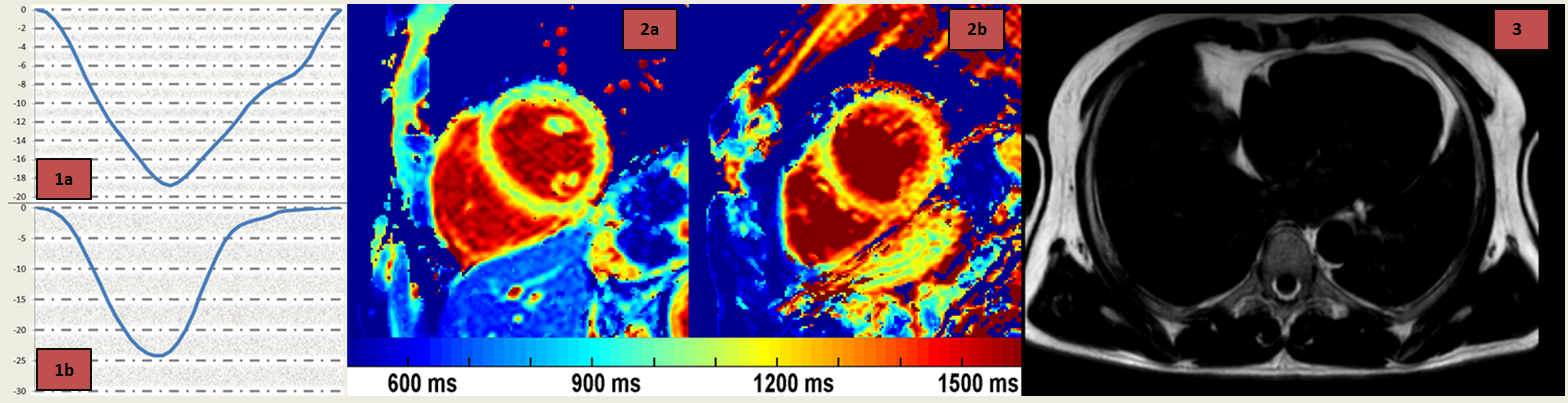
1: Lower longitudinal strain curve in a male hypertensive patient (a) compared to a healthy male (b)
2: The colors indicat higher T1-relaxation times in the hypertensive patient (b) compared to a healthy male (a).
3: Exemplary Dixon fat only image of a hypertensive male.