2751
Cardiac MR Derived Extracellular Volume Measurements Using Different Contrast AgentsAmir Ali Rahsepar1, Ahmadreza Ghasemiesfe1, Monica J Korell1, Jeremy D Collins1, and James C Carr1
1Department of Radiology, Northwestern University, Chicago, IL, United States
Synopsis
T1 and ECV values calculated from gadoterate meglumine enhanced CMR are comparable to more routinely used gadopentetate dimeglumine and gadobutrol CMR measurements.
Introduction
Cardiac magnetic resonance (CMR) is increasingly used to assess both macroscopic and microscopic myocardial scarring associated with a wide range of cardiac disease. Native and post-contrast T1 mapping CMR have been used to quantify myocardial fibrosis. Extracellular volume fraction (ECV) measurement has been considered to be a more robust method for quantifying myocardial fibrosis, particularly in diffuse interstitial processes affecting the myocardium. Linear Gadolinium-based contrast media have been traditionally used for delayed enhanced CMR; however with increased availability of macrocyclic Gadolinium based contrast agents, it is unclear what their influence is on scar detection as well as quantifiable imaging biomarkers. Moreover, recent reports have demonstrated that serial application of linear Gadolinium-based contrast agents (GBCA) increases the risk of Gadolinium retention, an effect not commonly associated with macrocyclic GBCA [1]. Due to the crucial role of microscopic scar detection at CMR, and the increasing use of macrocyclic agents, we aimed to compare ECV measurements using a macrocyclic GBCA (gadoterate meglumine, Dotarem, Guerbet, France) with another macrocyclic GBCA (gadobutrol, Gadovist, Bayer, Germany) and a linear GBCA (gadopentetate dimeglumine, Magnevist, Bayer, Germany).Methods
25 subjects (age: 60±10, 68% male) who underwent CMR using gadopentetate dimeglumine (n=8) or gadobutrol (n=17) were recruited. A research CMR scan was performed within an eight-week period using gadoterate meglumine on the same field strength (1.5 or 3-T) MR scanner as the clinical scan (Avanto/Skyra, Magnetom, Siemens, Germany). T1-mapping was performed using a modified Look-Locker inversion recovery (MOLLI) technique. Data for each slice (base, mid, apex) were acquired during breath holding pre- and 12–25 minutes following the intravenous administration of extracellular Gd-contrast (0.2 mmol/kg). Imaging reconstruction included motion correction of the MOLLI images with different inversion times, and the calculation of parametric LV T1 maps. The patient’s hematocrit was collected before the CMR exam. T1 mapping pre- and post-contrast images were measured segmentally based on the AHA 16-segment model and extracellular volume fraction (ECV) was calculated for all subjects using commercially available software (Circle 5.3, Calgary, Canada) (Figure 1). The average ECV values were calculated for all basal, mid and apical LV slices. Quantitative differences in scar between the two agents were assessed using Bland-Altman plots. Intraclass correlation coefficient (ICC) and the Wilcoxon signed rank test were used to check for reliability and differences in qualitative ratings between myocardial scar using the two GBCAs.Results
Overall, 25 subjects (58.9 ± 12.74 years, 68% men) with a variety of cardiac diseases (e.g. myocarditis, myocardial infarction) were enrolled in this study. Averaged native T1 values in the first and second MRI scan was 991.5±87 and 1013.7±50.4 msec at 1.5T and 1132.5±138 and 1249.7±42.1 msec at 3T. The reliability of native T1 values between the first and second scan was very good (ICC=67.7%). The ECV map of a patient with massive myocardial infarction using gadobutrol and gadoterate meglumine is shown in Figure 2. Average ECV for patients who received gadopentetate dimeglumine and gadoterate meglumine were 28.7±2.9% vs. 28.85±2.64%, with excellent reliability (Intraclass correlation of 0.947). Average ECV for patients who received gadobutrol and gadoterate meglumine were 28.73±4.92% vs. 28.53±4.59% with excellent reliability (Intraclass correlation of 0.967). Bland-Altman plot of the difference in ECV measurement between gadoterate meglumine and gadopentetate dimeglumine and gadobutrol and gadoterate meglumine did not show any systematic difference (Figure 3).Conclusion
The results of this study indicate that T1 and ECV values calculated from gadoterate meglumine enhanced CMR are comparable to more routinely used gadopentetate dimeglumine and gadobutrol CMR measurements. With increasing utilization of macrocyclic contrast agents in MRI generally, their use in CMR appears to yield comparable quantitative results to linear agents in this small patient centered study.Acknowledgements
This work was funded by Gerubet, LLC.References
[1] Radbruch et al. Gadolinium Retention in the Dentate Nucleus and Globus Pallidus is dependent on the class of contrast agent. Radiology 2015.Figures
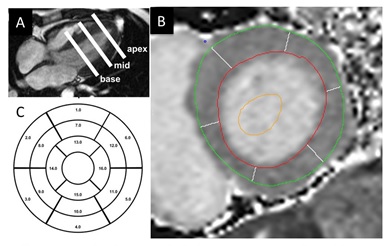
T1 mapping for ECV evaluation. MOLLI was performed in
basal, mid, and apical LV (A). LV epi- and endocardial contours were manually
drawn (B). Using 16-segment model, regional and global T1 and ECV was
calculated.
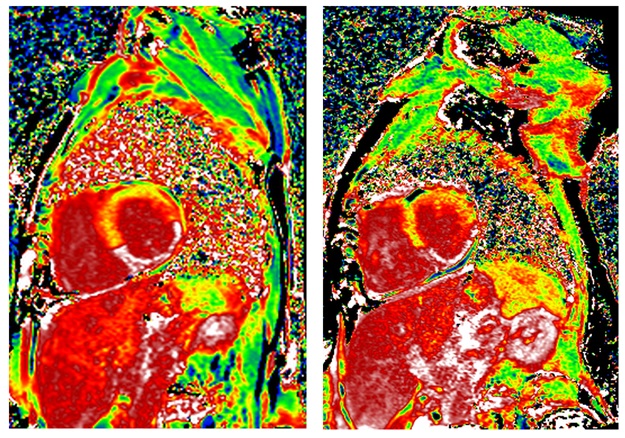
Similar ECV map and ECV measurement
of a patient with massive myocardial infarction using gadobutrol (ECV=40.5%, left) and gadoterate
meglumine (ECV=41.2%,
right).
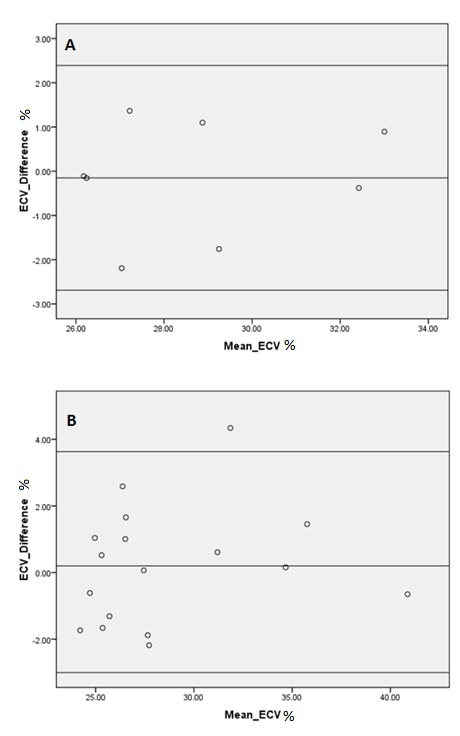
Bland-Altman
plot of difference in ECV measurement between gadoterate meglumine and
gadopentetate dimeglumine (A) and gadobutrol and gadoterate meglumine (B).