2730
Gender-based optimization of cardiac follow up in thalassemia major patients1Fondazione G. Monasterio CNR-Regione Toscana, Pisa, Italy, 2CMR Unit, Fondazione G. Monasterio CNR-Regione Toscana, Pisa, Italy, 3"ARNAS" Civico, Di Cristina Benfratelli, Palermo, Italy, 4Azienda Ospedaliera "Garibaldi" Presidio Ospedaliero Nesima, Catania, Italy, 5Fondazione di Ricerca e Cura "Giovanni Paolo II", Campobasso, Italy, 6Presidio Ospedaliero ASL 5, Crotone, Italy, 7Ospedale “Giovanni Paolo II”, Olbia, Italy
Synopsis
Females seem to tolerate iron toxicity better, possibly as an effect of reduced sensitivity to chronic oxidative stress. Based on our data about the significantly different risk in developing cardiac complications, in females older than 20 years the FU may be performed every 24 months, thus optimizing health care costs.
Purpose
We prospectively assessed in a large and multicenter cohort of thalassemia major (TM) patients if the male gender was associated with an higher risk of cardiac iron accumulation, myocardial fibrosis and heart dysfunction assessed by CMR and cardiac complications (heart failure, arrhythmias and pulmonary hypertension) in order to optimize the timing in cardiac follow up (FU).Methods
We considered 1711 TM patients (899 females, 31.09±9.08 years), consecutively enrolled in the Myocardial Iron Overload in Thalassemia (MIOT) Network.1 Myocardial iron overload was assessed by the multislice multiecho T2* technique.2 Biventricular function was quantified by cine images.3 Late gadolinium enhancement (LGE) images were acquired to detect myocardial fibrosis.4Results
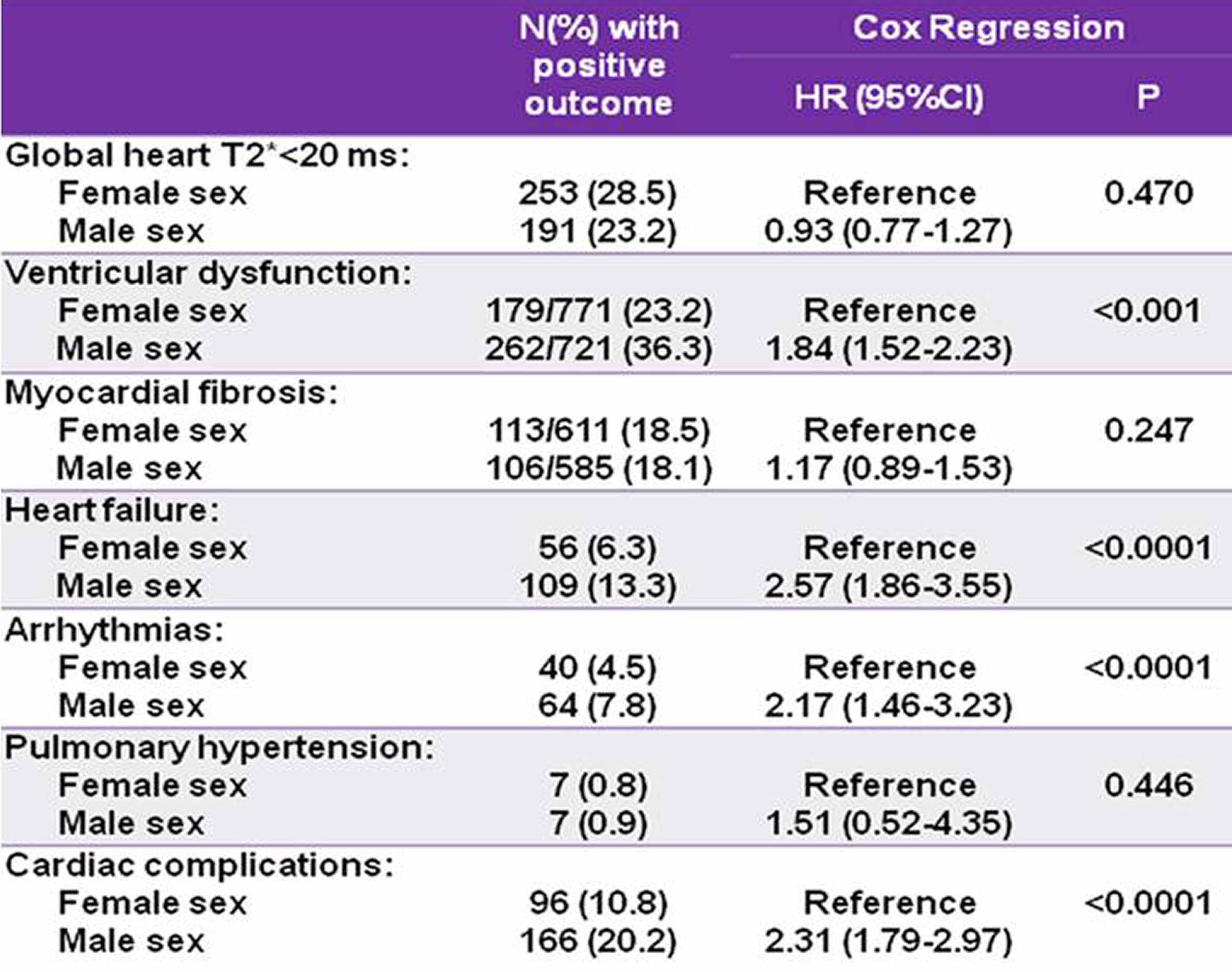
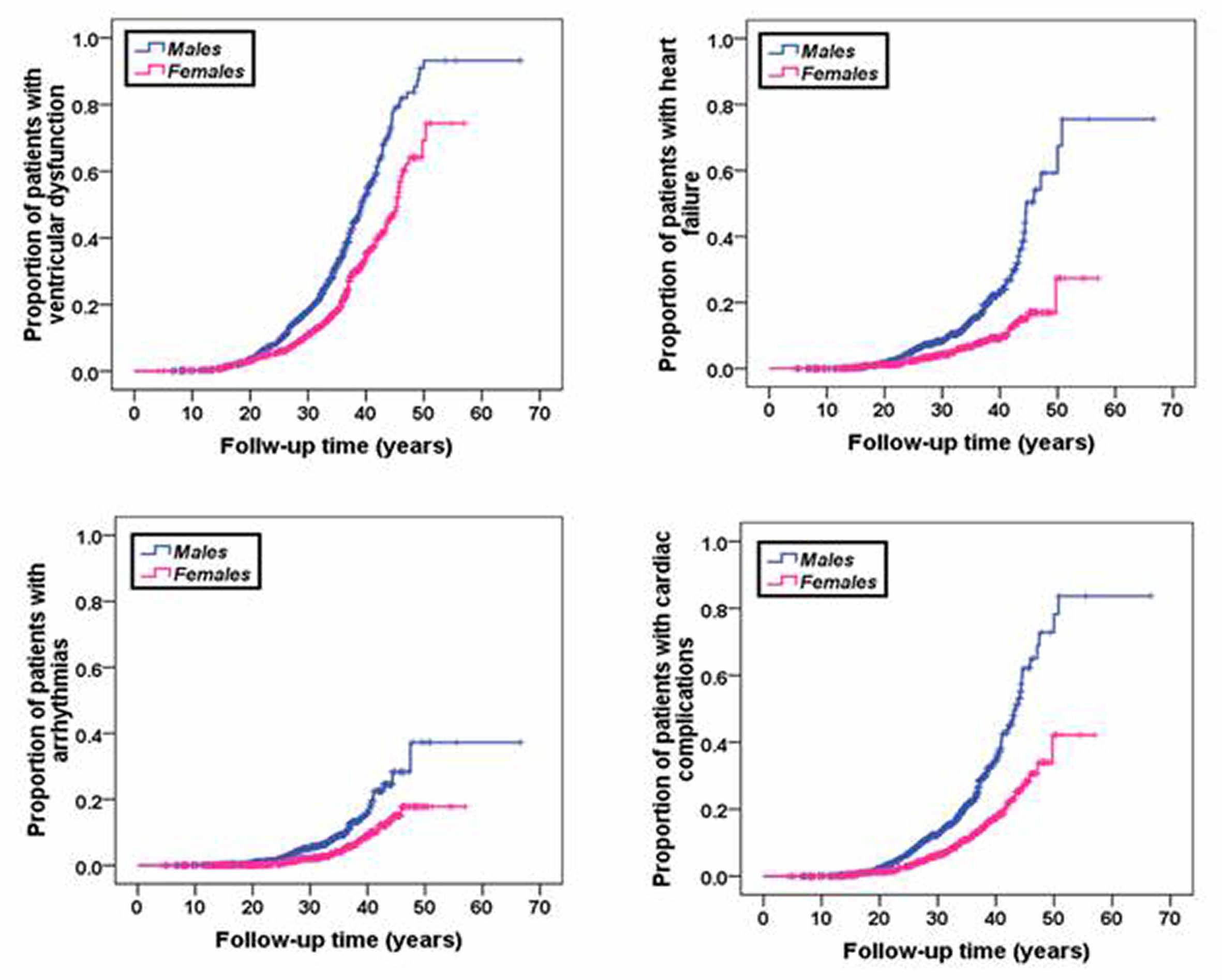
Although having a similar risk of accumulating iron, males showed a significant higher risk of developing cardiac dysfunction, heart failure, arrhythmias and cardiac complications globally considered (Table 1). Figure 1 shows the Kaplan-Meier curves for the outcomes for which the male sex was a significant prognosticator. Looking at the Kaplan-Meier curves, a peculiarity leaped out: until 20-30 years of follow-up the two lines (male and female sex) were almost overlapping while after they clearly diverged.
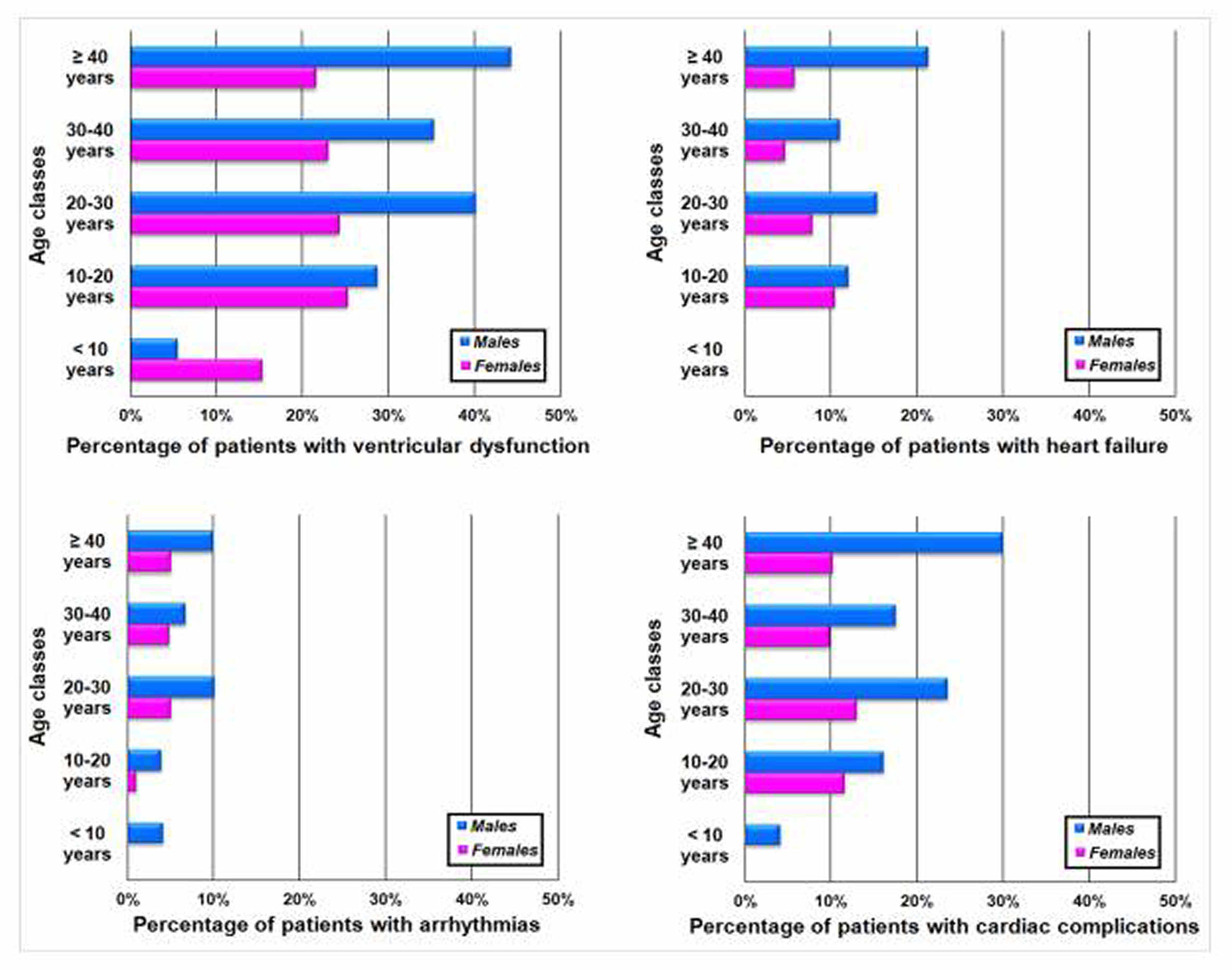
Patients were divided in groups based on the follow-up duration: <10 years, between 10 and 20 years, between 20 and 30 years, between 30 and 40 years and ≥40 years. Figure 2 shows that a significant gender-specific difference in the frequency of ventricular dysfunction and cardiac complications appeared for patients followed for at least 20 years. So, two subgroups of patients were identified: patients followed for less than 20 years and patients followed for more than 20 years. In the first subgroup males and females had a comparable risk of developing cardiac iron overload, ventricular dysfunction and cardiac complications. Conversely, if a follow-up longer than 20 years was considered, males exhibited a significant higher risk of having ventricular dysfunction, heart failure, arrhythmias, and cardiac complications.
Conclusion
Females seem to tolerate iron toxicity better, possibly as an effect of reduced sensitivity to chronic oxidative stress.
According to National and International Guidelines,5,6 in thalassemia major patients without cardiac involvement ECG, echocardiography, 24-h ECG and CMR should be performed annually. In the definition of this timing, the possible difference between males and females in the risk of development of cardiac diseases was not taken into account. In this context, the present study may help to redefine the timing of the cardiologic screening, diversified based on patients gender. This is important since health care budgets around the world are being squeezed and optimized expenses represents a top priority for the health systems. Based on the results of the present study, we suggest the following timelines for TM patients. The first complete cardiac evaluation should be performed as soon as possible and, until the 20 years of age, the cardiologic follow-up should be performed annually for all. Over 20 years of age, males should carry on with the annual follow-up while females, having an about 50% lower risk of cardiac diseases, could perform a complete cardiologic assessment every 2 years, in absence of pathological findings. Considering the costs of every diagnostic tool, our proposed approach could allow to save 698.35 Euros/year for each female patient.
Acknowledgements
No acknowledgement found.References
1. Meloni A, Ramazzotti A, Positano V, et al. Evaluation of a web-based network for reproducible T2* MRI assessment of iron overload in thalassemia. Int J Med Inform. 2009;78(8):503-512.
2. Pepe A, Positano V, Santarelli F, et al. Multislice multiecho T2* cardiovascular magnetic resonance for detection of the heterogeneous distribution of myocardial iron overload. J Magn Reson Imaging. 2006;23(5):662-668.
3. Aquaro GD, Camastra G, Monti L, et al. Reference values of cardiac volumes, dimensions, and new functional parameters by MR: A multicenter, multivendor study. J Magn Reson Imaging. 2016.
4. Pepe A, Positano V, Capra M, et al. Prevalence and clinical-Instrumental correlates of myocardial scarring by delayed enhancement cardiovascular magnetic resonance in thalassemia major. Heart. 2009;95:1688-1693.
5. Cogliandro T, Derchi G, Mancuso L, et al. Guideline recommendations for heart complications in thalassemia major. J Cardiovasc Med (Hagerstown). 2008;9:515-525.
6. Pennell DJ, Udelson JE, Arai AE, et al. Cardiovascular function and treatment in beta-thalassemia major: a consensus statement from the American Heart Association. Circulation. 2013;128:281-308.
Figures