2729
The prognostic role of hypertrabeculation by cardiac magnetic resonance in thalassemia intermedia patients1Fondazione G. Monasterio CNR-Regione Toscana, Pisa, Italy, 2Università degli Studi di Palermo, Policlinico "Paolo Giaccone", Palermo, Italy
Synopsis
We prospectively assessed whether the Piga’s criterion for left ventricle non-compaction (LVNC) (NC/C ratio threshold of >2.5) had a prognostic role for adverse cardiovascular outcomes in thalassemia intermedia patients. We found out that patients with Piga’s positive criterion had a significant higher risk of developing cardiac complications globally considered and arrhythmias.
Purpose
Differentiation of left ventricle non-compaction (LVNC) from hypertrabeculated LV due to a negative heart remodeling in thalassemia intermedia (TI) can depends on the selected CMR criterion. The recently proposed Piga’s criterion1 (NC/C ratio threshold of >2.5) seems to have a low specificity to identify the true LVNC in TI. Anyway, the Piga’s criterion could well detect easy a negative heart remodeling in TI patients.
The aim of this study was to prospectively assess whether the Piga’s criterion has a prognostic role for adverse cardiovascular outcomes in TI patients.
Methods
We considered 168 TI patients (86 males, mean age 38.44±11.52 years) consecutively enrolled in the Myocardial Iron Overload in Thalassemia (MIOT) Network.2
Cine steady-state free precession sequences were acquired on long-axis two-chamber, four-chamber, three-chamber and short-axis views to cover the whole LV without any gap between images. The images were transferred to a dedicated workstation. For the evaluation of the NC/C ratio, a 16-segment model of the LV3 was used. At each segment, the thickness of the non-compacted and the compacted myocardium was measured perpendicular to the long-axis direction of the compacted myocardium at end-diastole and the NC/C ratio was calculated. The maximal NC/C ratio was then used for diagnosis.
Myocardial iron overload was assessed by the multislice multiecho T2* technique.4 Biventricular function was quantified by cine images using MASS software.5 Late gadolinium enhancement (LGE) images were acquired to detect myocardial fibrosis.6
Results
Seven patients were excluded because a cardiac complication was present at the first CMR. Using Piga’s criterion the study population was divided into two groups: patients with Piga’s positive criterion (n=15, 9.3%) and with Piga’s negative criterion (n=146, 90.7%).
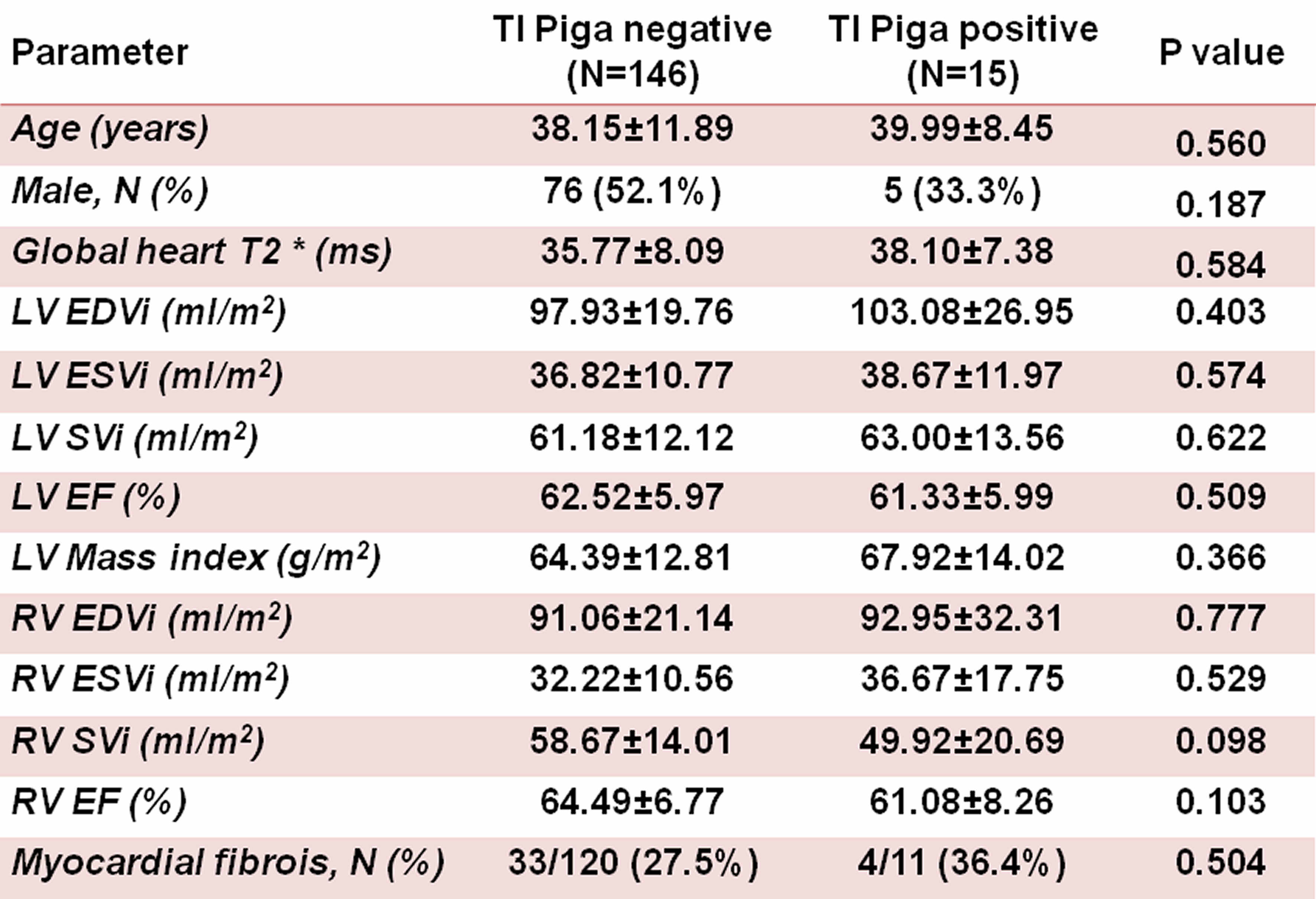
Table 1 shows the comparison of basal CMR data. Cardiac iron, biventricular function and frequency of myocardial fibrosis were comparable between the two groups.
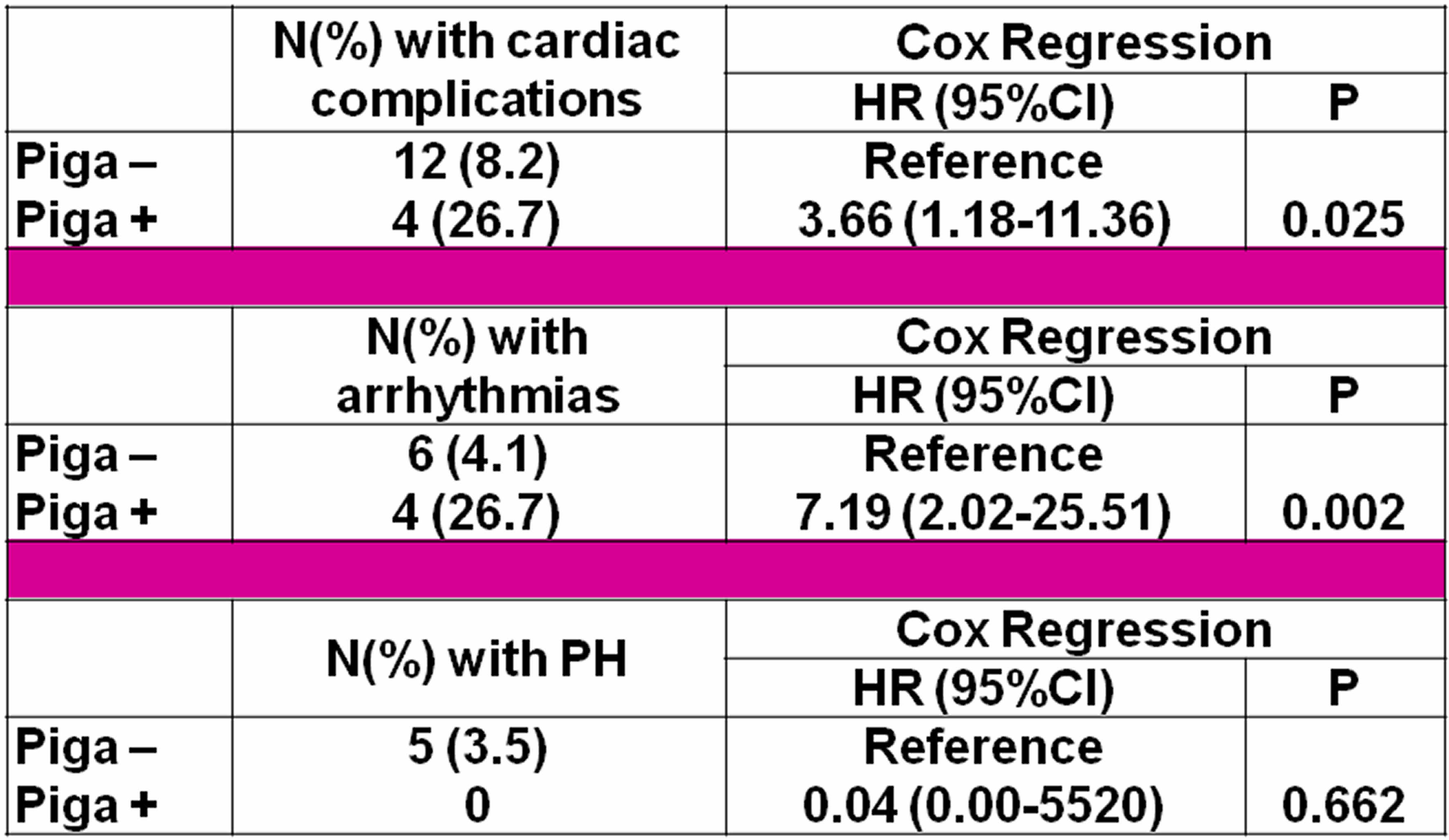
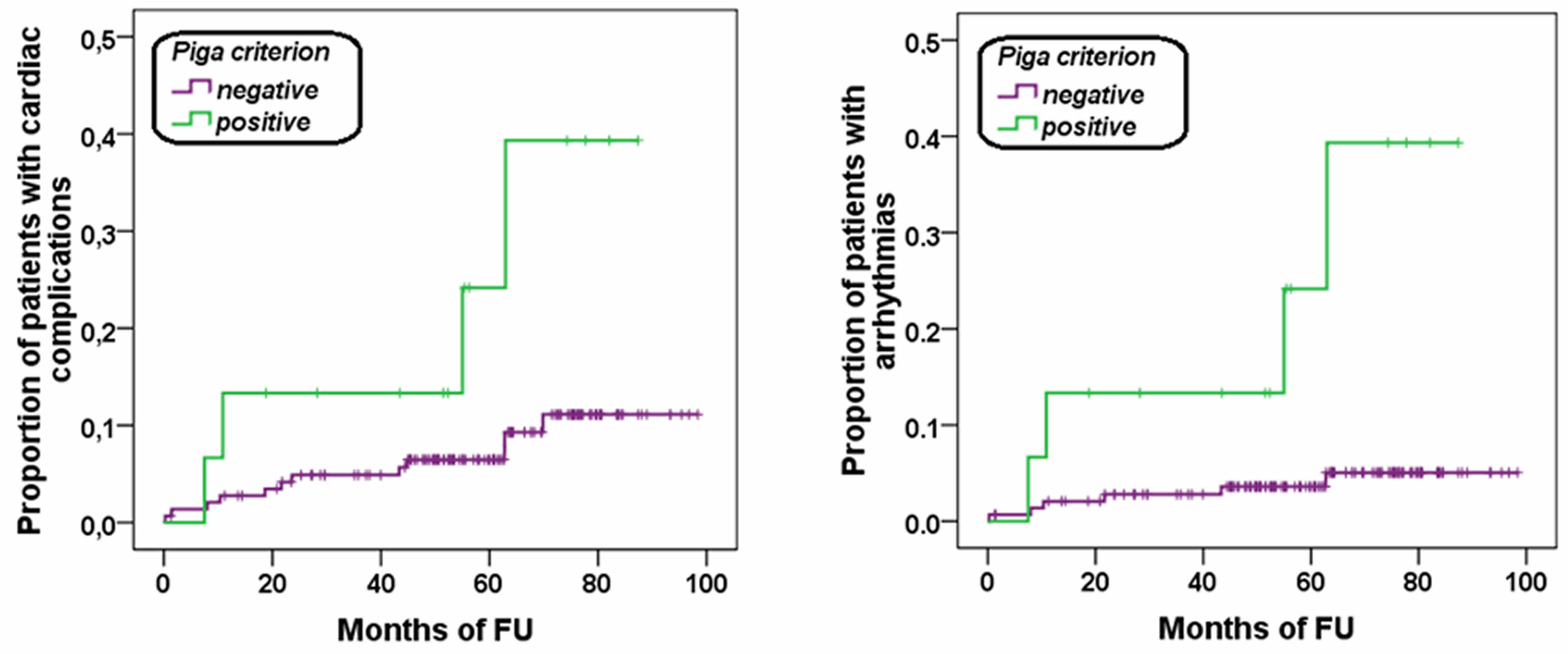
Mean follow-up time was 57.50± 21.86 months. Sixteen new cardiac events were recorded: 1 heart failure (HF), 10 supraventricular arrhythmias and 5 pulmonary hypertension (PH). The patients with Piga’s positive criterion had a significant higher risk of developing cardiac complications globally considered and arrhythmias (Table 2). Figure 1 shows the Kaplan-Meier survival curves.
Fourteen patients had a prior and resolved history of cardiac disease. The HR for previous cardiac diseases predicting future complications was 7.04 (95%CI=2.56-19.40; P<0.0001). In the multivariate model the independent predictive factors were: Piga’s positive criterion (HR=3.72, 95%CI=1.19-11.67, P=0.024) and previous cardiac complications (HR=7.09, 95%CI=2.57-19.53, P<0.0001).
Seven patients had a prior and resolved history of arrhythmias. The HR for previous arrhythmias predicting future arrhythmias was 16.80 (95%CI=4.24-66.57; P<0.0001). In the multivariate model the independent predictive factors were: Piga’s positive criterion (HR=9.49, 95%CI=2.49-36.27, P=0.001) and previous arrhythmias (HR=23.67, 95%CI=5.37-104.41, P<0.0001).
Conclusion
Based on our data a NC/C ratio >2.5 provides prognostic information for patients with TI.Acknowledgements
No acknowledgement found.References
1. Piga A, Longo F, Musallam KM, et al. Am J Hematol. 2012;87(12):1079-1083.
2. Meloni A, Ramazzotti A, Positano V, et al. Int J Med Inform. 2009;78(8):503-512.
3. Cerqueira MD, Weissman NJ, Dilsizian V, et al. Circulation. 2002;105(4):539-542.
4. Pepe A, Positano V, Santarelli F, et al. J Magn Reson Imaging. 2006;23(5):662-668.
5. Aquaro GD, Camastra G, Monti L, et al. J Magn Reson Imaging. 2016; in press.
6. Pepe A, Positano V, Capra M, et al. Heart. 2009;95:1688-1693.
Figures