2633
Parallel Transmission for Heating Reduction in Realistic Deep Brain Stimulation Lead Trajectories1University of Toronto, Toronto, ON, Canada, 2Massachusetts General Hospital, MA, United States, 3US Food and Drug Administration, Silver Spring, MD, United States, 4Sunnybrook Health Sciences Centre, ON, Canada, 5Innovere Medical, ON, Canada
Synopsis
Implanted devices for deep brain stimulation (DBS) create a safety concern during MRI due to heating at exposed tip of the lead. Parallel transmit (pTx) can potentially reduce heating of the lead tip when radiofrequency (RF) inputs are selected by an appropriate numerical optimization method. To date, however, this method has not considered how the trajectory of DBS leads affects heat deposition. The present work investigates the optimized pTx method for realistic DBS lead trajectories estimated from intra-operative computed tomography (CT) scans of nine patients, with simulations indicating statistically significant reduction in heating at lead tips while maintaining reasonable B1+-field homogeneity.
Purpose
Patients with deep brain stimulators (DBS) may be subject to localized heating during MRI due to interaction with excitatory radiofrequency (RF) fields. Parallel RF transmit (pTx)1 has been proposed to minimize such RF-induced heating in preliminary proof-of-concept studies2,3. In the clinic, lead trajectories differ substantially between patients depending on stimulation target and surgical implementation4. Lead trajectory is an important factor in the extent of RF coupling and in the input parameters required for pTx optimization. The present work evaluates the efficacy of the proposed pTx technique on realistic lead trajectories obtained from nine DBS patients.Methods
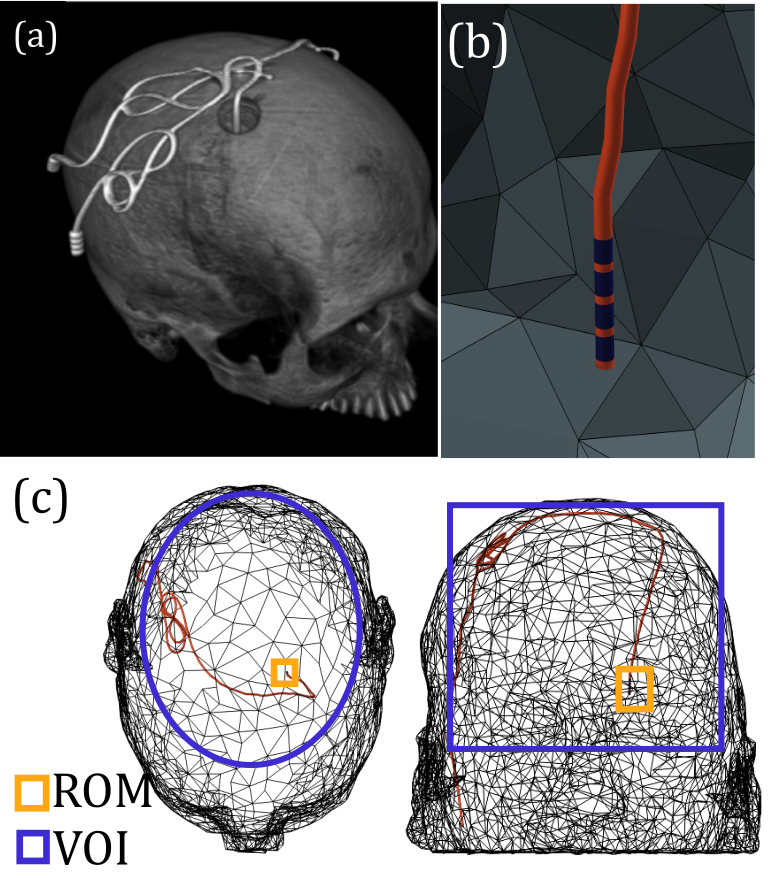
Nine patient-trajectory models were created from semi-automatically segmented intra-operative CT scans of patients implanted with DBS devices at Massachusetts General Hospital (MGH). The sub-thalamic nucleus was the DBS target in all cases. Use of patient data for modeling and simulation was approved by the Internal Review Board of MGH. Lead trajectories were obtained using an intensity histogram to determine the location of the hyperdense DBS lead. A skeletonization algorithm was then implemented to determine the center line of the lead, which was expanded into an insulated DBS lead model with four exposed electrodes (Fig. 1).
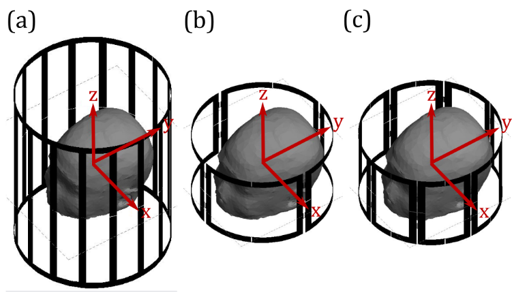
Electromagnetic simulations were performed in FEKO software using 4- and 8-element pTx coils compared with standard transmit/receive birdcage coil excitation (Fig. 2). For each patient, optimization was performed using a Simplex algorithm in Matlab to minimize local SAR in a region of minimization (ROM) surrounding a DBS lead tip and the inhomogeneity of the B1+-field within a volume of interest (VOI) by varying the input amplitude and phase for each coil element (Eq. 1).
$$ \min_{A_n,\phi_n}(\frac{\sigma_{VOI}(\mid B_{1,tot}^+\mid )}{\mu_{VOI}(\mid B_{1,tot}^+\mid )}+\lambda\cdot \mu_{ROM}\frac{\mid E_{tot}\mid^2}{\mid E_{quad}\mid^2}) ( 1 )$$
where σVOI (∙) is the standard deviation over the VOI; μVOI (∙) and μROM (∙) are the mean over the VOI and the ROM, respectively; λ is a weighting factor used to control the relative importance of safety (through the E-field term) and image quality (through the B1+-field term); and Equad is the E-field in pTx quadrature mode (An=1, φn=2π/N). The ROM and VOI are defined for each patient (Fig. 1).
The weighting factor λ was chosen individually for each patient to increase the degrees of freedom of the optimization and improve solutions. Solutions were rejected that violated a pre-determined 1 g SAR safety limit of 0.4 W/kg, which represents a 75 % decrease in 1 g SAR compared with the median birdcage coil excitation. The remaining solutions were separated into 5 % intervals of the coefficient of variation (COV) of the B1+-field. The minimum COV value was chosen among 5 % intervals within chosen SAR safety limit.
Results
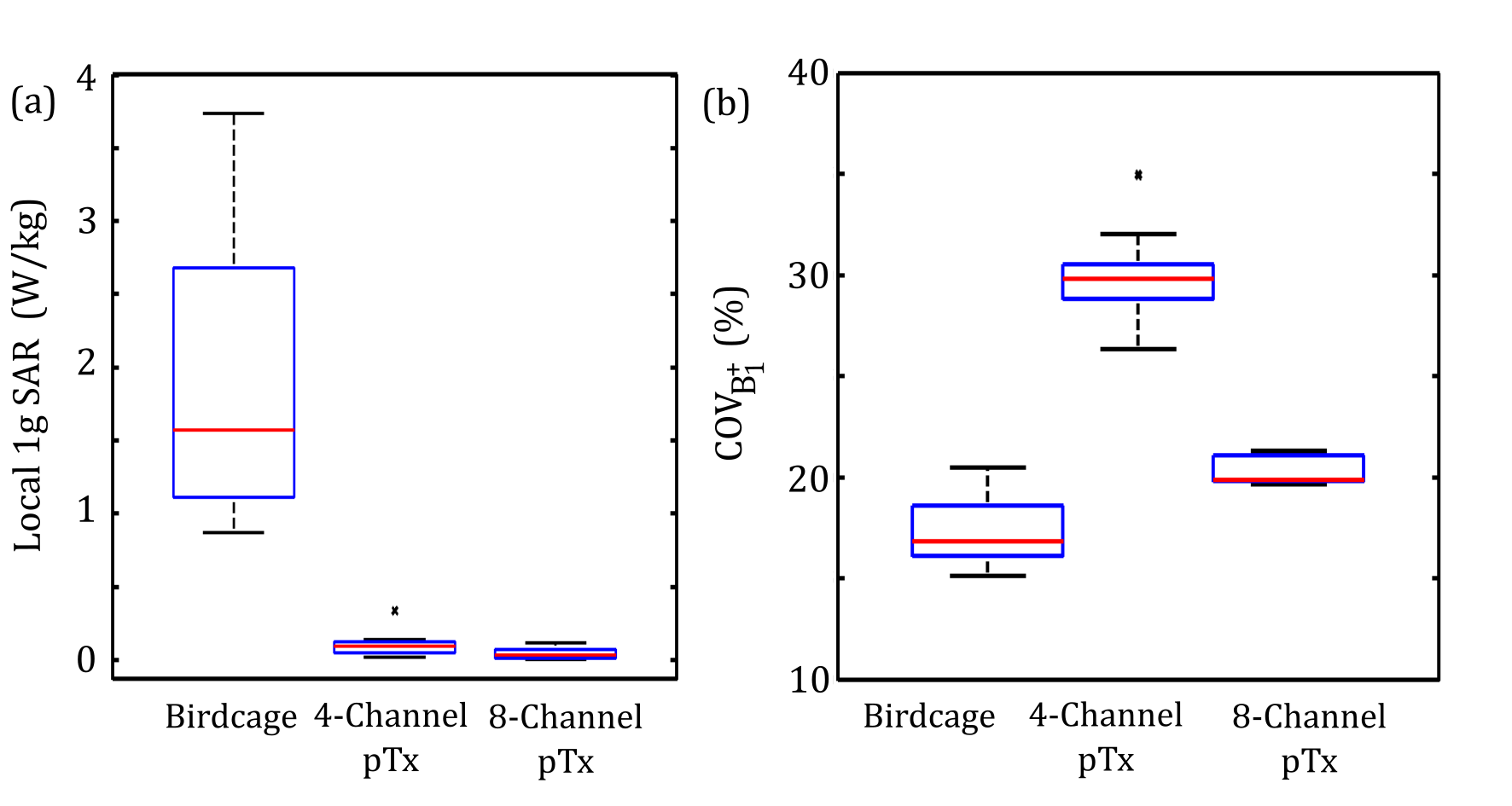
The median and interquartile range for a) local SAR and b) COV of the B1+ field is shown in Fig. 3 for each RF coil configurations. Statistical significance was determined using the Wilcoxon signed rank test at p < 0.05. Local SAR was significantly reduced at the lead tip with both 4-element and 8-element pTx with a median decrease of 94 % and 97 %, respectively. The median COV of B1+ inhomogeneity was increased to a value of 30 % for 4-element pTx and 20 % for 8-element pTx compared to a value of 17 % for the birdcage coil.
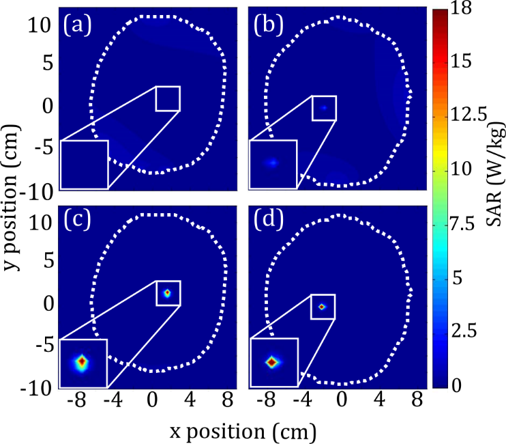
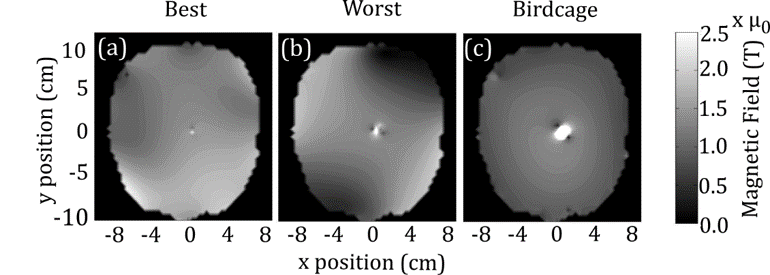
Figures 4 and 5 show the local SAR and B1+-field in the axial slice through the lead tip of “best” and “worst” patient results with pTx, and the birdcage coil results for these patients. “Best” results (lowest local SAR and highest B1+ homogeneity) were obtained with 8-element pTx, whereas “worst” results (highest local SAR and lowest B1+ homogeneity) were obtained with 4-element pTx. Worst-case local SAR with 4-element pTx was still markedly reduced compared to birdcage excitation, with acceptable B1+ homogeneity near the lead tip.
Discussion
Large variation in 1 g SAR was observed for excitation with the birdcage coil (Fig. 3) as expected4. In general, 8-element pTx performed better than 4-element pTx with statistically significant gains in B1+ homogeneity. Utilizing a pre-existing CT scan to tailor this pTx technique to each patient may be possible in the future, but considerably more work is required to develop a practical pTx imaging implementation that accounts for the wide range of expected DBS lead trajectories, includes on-line safety monitoring, and enables pTx inputs to be incrementally adjusted as needed at scan time.Conclusion
Simulations involving nine DBS patient models suggest that optimized pTx provides a robust approach to minimizing local SAR with respect to lead trajectory.Acknowledgements
No acknowledgement found.References
1. Katscher U, Bornert P, Leussler C, van den Brink JS. Transmit SENSE. Magn Reson Med 2003; 49(1):144-50.
2. Eryaman Y, Guerin B, Akgun C, Herraiz JL, Martin A, Torrado-Carvajal A, Malpica N, Hernandez-Tamames JA, Schiavi E, Adalsteinsson E, et al. Parallel transmit pulse design for patients with deep brain stimulation implants. Magn Reson Med 2015; 73(5):1896-903.
3. McElcheran CE, Yang B, Anderson KJ, Golenstani-Rad L, Graham SJ. Investigation of Parallel Radiofrequency Transmission for the Reduction of Heating in Long conductive Leads in 3 Tesla Magnetic Resonance Imaging. PLoS One 2015; 10(8):e0134379.
4. Mattei E, Triventi M, Calcagnini G, Censi F, Kainz W, Mendoza G, Bassen HI, Bartolini P. Complexity of MRI induced heating on metallic leads: experimental measurements of 374 configurations. Biomed Eng online 2008; 7(1):11.
Figures