2612
Artifact-reduced imaging of biopsy needles with 2D multi-spectral imaging1Radiology, Stanford University, Stanford, CA, United States
Synopsis
MR-guidance for biopsy procedures features high intrinsic soft-tissue contrast. However, artifacts induced by the metallic needle can reduce the localization of the needle and require low susceptibility needle materials with poorer cutting performance. In this work, we explore 2D multi-spectral imaging (2DMSI) for reducing the needle artifacts for more precise needle localization and tracking or to enable the usage of conventional stainless-steel biopsy needles.
Purpose
To evaluate the ability of 2D multi-spectral imaging (2DMSI) for artifact-reduced imaging of both MR-compatible and conventional biopsy needles.Introduction
MRI enables guidance of biopsy procedures with high intrinsic soft-tissue contrast. However, the metallic needle can induce field inhomogeneities, resulting in artifacts such as distortions or signal void due to dephasing in gradient-recalled echo (GRE) sequences conventionally used for guidance [1]. Though signal voids may aid in localizing the needle, this makes it challenging to pinpoint the exact needle location for reliable targeting of smaller lesions. In-plane and through-plane distortions can misguide the needle path, as lesions might appear at a different position on imaging with respect to their actual location. “MR compatible”, low susceptibility materials such as cobalt-chromium, nickel-chromium or titanium can reduce these artifacts. However, these materials are a significant compromise for biopsy, as they cannot be ground as sharply, resulting in a poor cutting performance and sample quality.
2DMSI enables imaging in the presence of strong field inhomogeneities by segmenting the slice into spectral regions (“bins”) that can be imaged with minimal artifact [2] (Fig. 1). In this work, we use 2DMSI to both virtually remove the artifacts for MR compatible needles and to reduce the artifacts for a conventional stainless steel needle to an acceptable level. We further explore the 2DMSI-intrinsic off-resonance information for tracking of the needle.
Methods
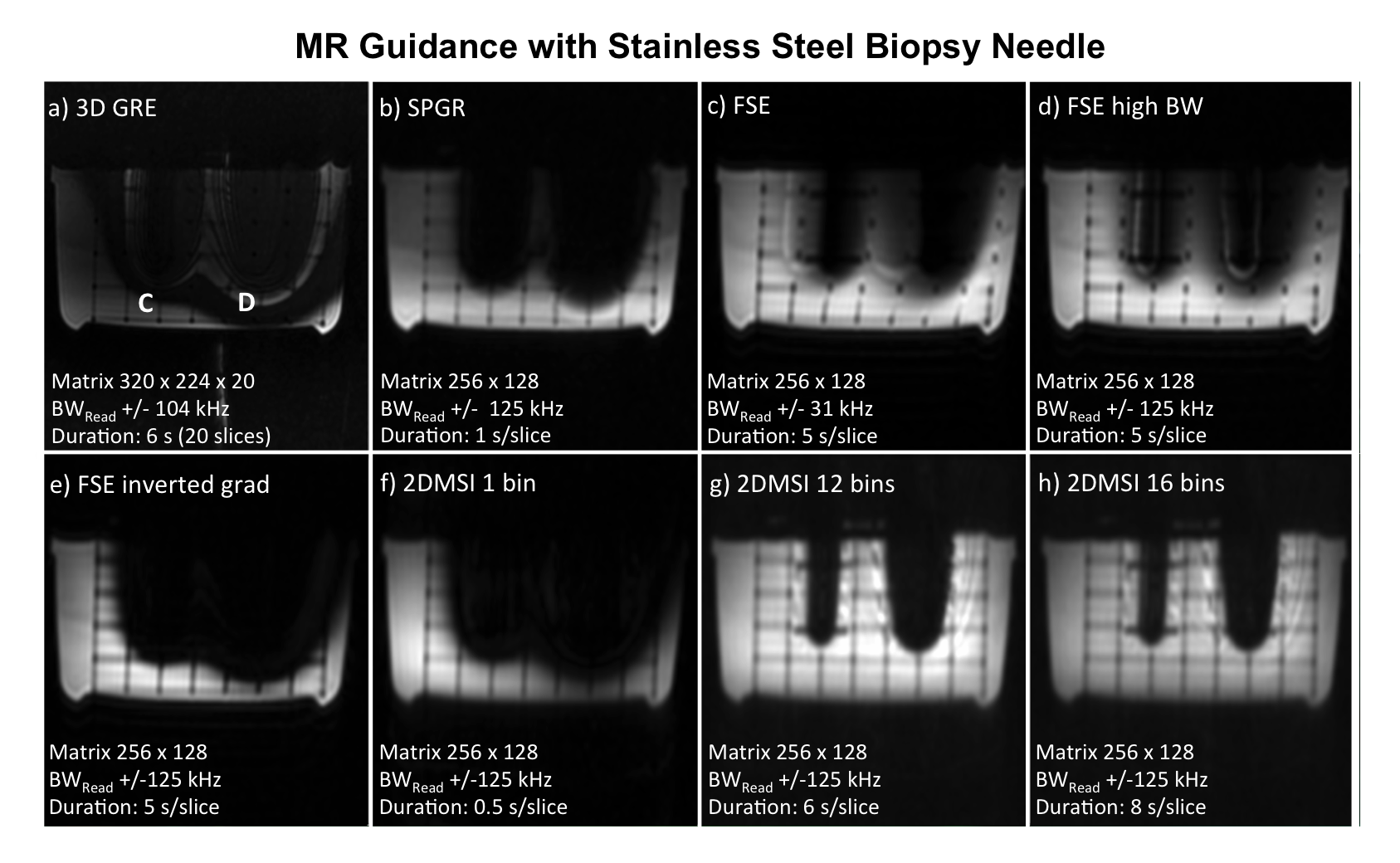
Imaging experiments were performed on a 3T human MRI using a 6 channel surface coil. The needles (see Fig. 2 for details) were mounted in a rectangular plastic grid and immersed in water. All needles were oriented perpendicular to the static magnetic field to maximize artifact. To compare with conventional imaging and alternative artifact reduction techniques, axial images were acquired with single-shot 2DMSI, fast-spin-echo (FSE), spoiled-gradient-recalled-echo (SPGR) and 3D gradient-echo (3D GRE). Sequence-specific details are listed in Fig. 3. FSE imaging was repeated with increased readout bandwidth and inverted slice selection gradient [3]. 2DMSI images were acquired with 1 bin (covering off-resonances from -0.5kHz to 0.5kHz) 12 bins (-4.5kHz to 5.4kHz) and 16 bins (-6.3kHz to 7.2kHz, stainless-steel needle only).
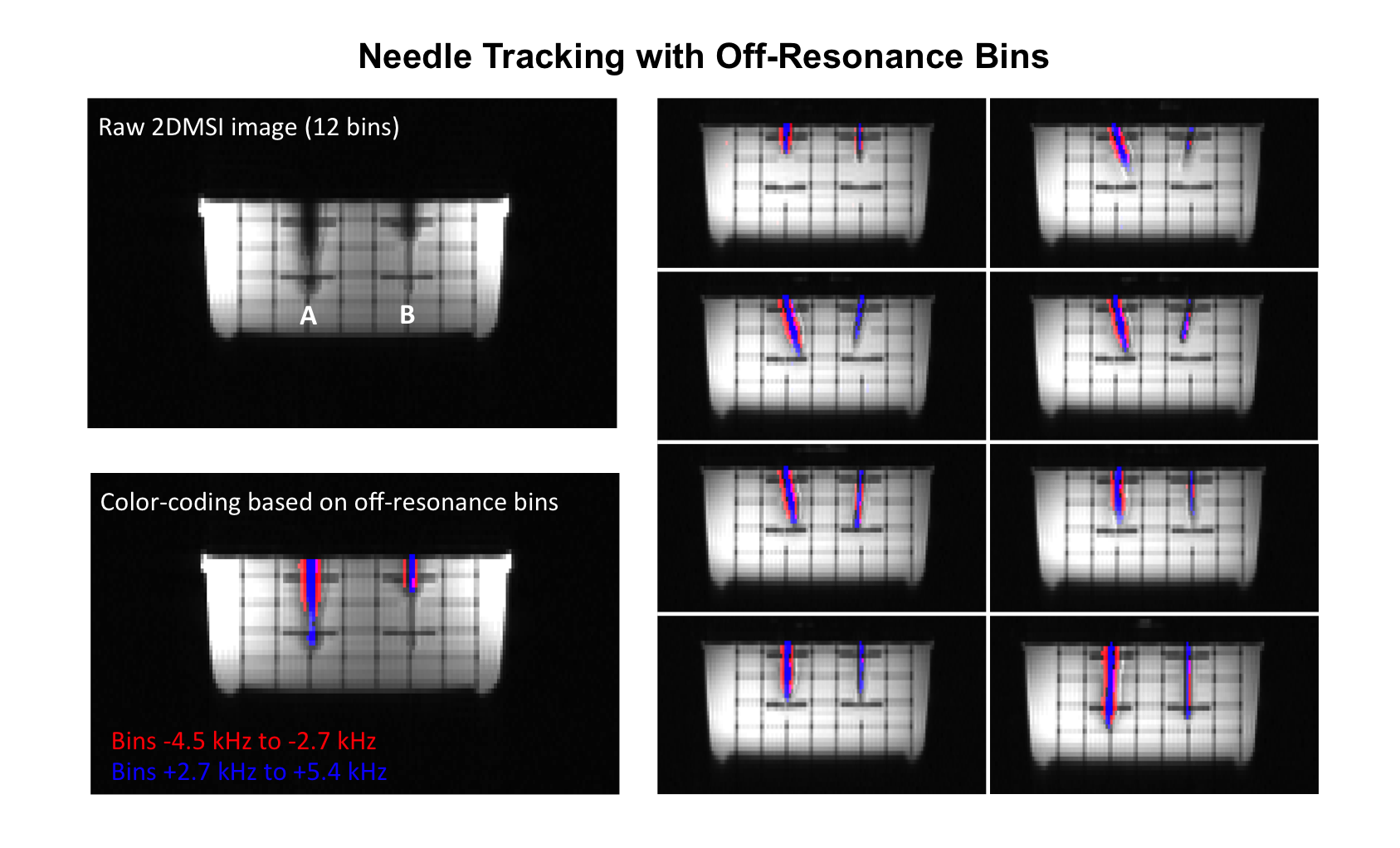
For needle tracking, the regions of the higher off-resonance bins were colored with respect to the sign of the off-resonance. The regions were determined from the signal intensity within the individual bin images by thresholding.
Results & Discussion
Figure 3 shows the axial slices through the axis of both MR-compatible needles. With all sequences, the needles are visible although the ability to pinpoint them varies strongly. Although the 3D GRE image (a) produces an easily visible needle axis, hypo- and hyper-intense signals surround the needle. Despite a comparable short TE of 1.9ms, the SPGR image (b) is dominated by signal void, limiting the ability to pinpoint the needle.
In comparison, the FSE image (c) compensates for signal void, revealing the distortions visible as hypo- and hyper-intense bands surrounding the needle. Increasing the readout bandwidth (d) reduces the in-plane distortions and the through-plane distortions become more distinct. Inverting gradients (e) successfully suppresses the signal from the distorted off-resonance region, identifying the unbiased signal. Single bin 2DMSI (f) reveals a similar result, although higher-bandwidth RF-pulses cause a better region selection. Adding off-resonance bins (g) reveals the regions close to both needles without distortions. Adjusting the number of bins therefore allows for choosing the coverage around the needle as a tradeoff between needle conspicuity and ability to pinpoint its location.
Figure 4 shows the results for the components of the stainless steel needle. Compared to the reference methods, 2DMSI strongly increases coverage close to the needles. In particular for the cannula (left), relevant for the cutting performance, the extent of the artifacts is comparable to the one for MR compatible needles with conventional imaging [1].
The results for the needle tracking using the bin off-resonance information are shown in Fig. 5. The red color and blue color mark the signal provided by the negative and positive off-resonance bins, respectively. Signal in the tip of the left needle is due to partial volume effects. Moving of the needle out the imaging plane would change the ratio between positive and negative off-resonances.
Conclusions
2DMSI shows promising results for both artifact-reduced imaging of biopsy needles for a more precise needle localization and needle tracking. 2DMSI might be of particular promise for biopsy needles inducing large distortions or for targeting of small lesions. In addition, it may enable use of a wider range of needle materials, with potentially better sampling performance.Acknowledgements
This work was supported by NIH (R01 EB017739, R21 EB019723, P01 CA159992) and GE Healthcare.References
[1] Penzkofer T, Peykan N, Schmidt K, Krombach G, Kuhl CK. How MRI Compatible is “MRI Compatible”? A Systematic Comparison of Artifacts Caused by Biopsy Needles at 3.0 and 1.5 T. Cardiovasc Intervent Radiol. 2013;36:1646-1657.
[2] Hargreaves BA, Taviani V, Yoon D. Fast 2D Imaging for Distortion Correction Near Metal Implants. Proc ISMRM 22. 2014, #615.
[3] Butts K, Pauly JM, Daniel BL, Kee S, Norbash AM. Management of Biopsy Needle Artifacts: Techniques for RF-Refocused MRI. J Mag Res I. 1999;9:586-595.
Figures
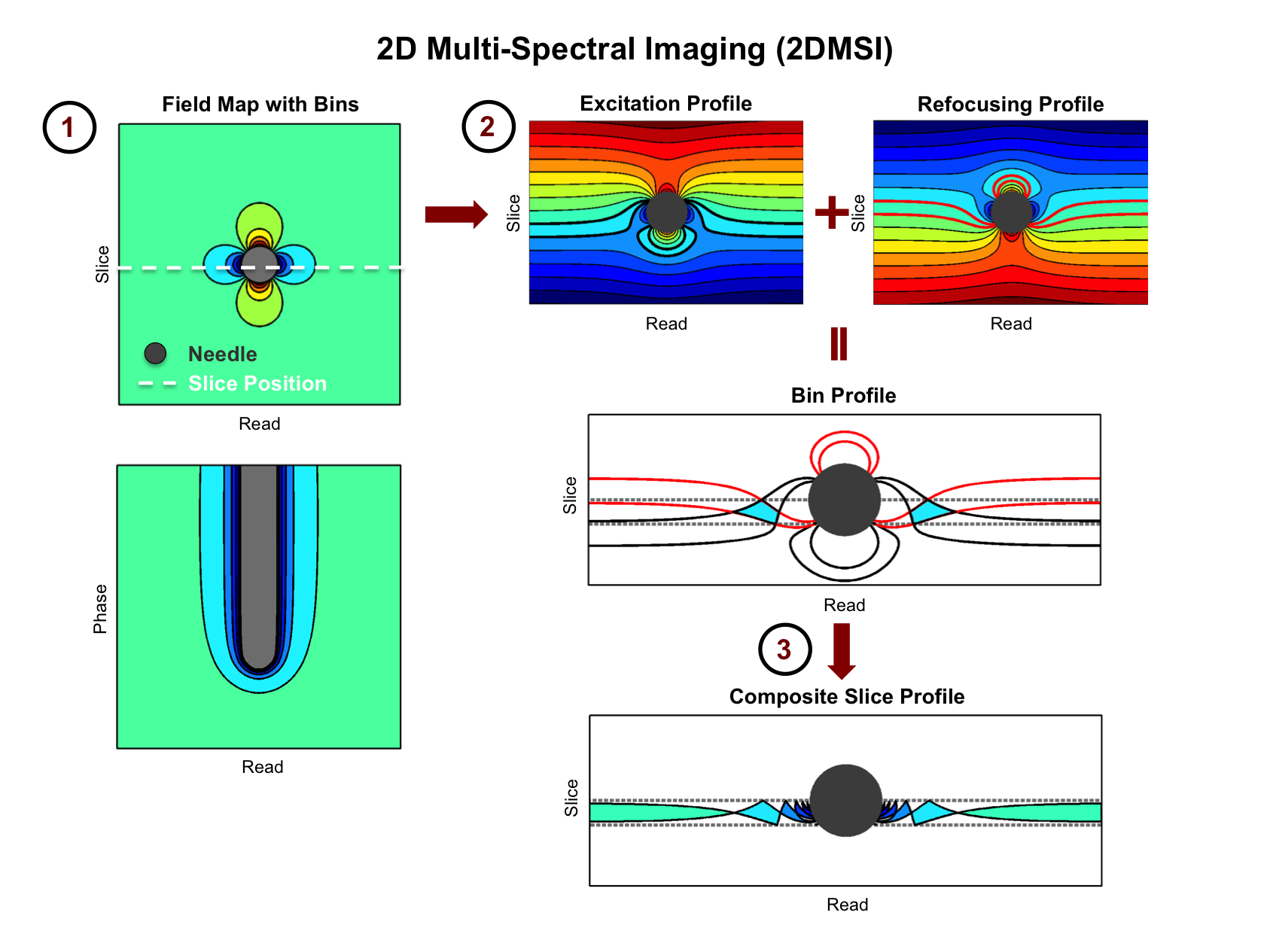
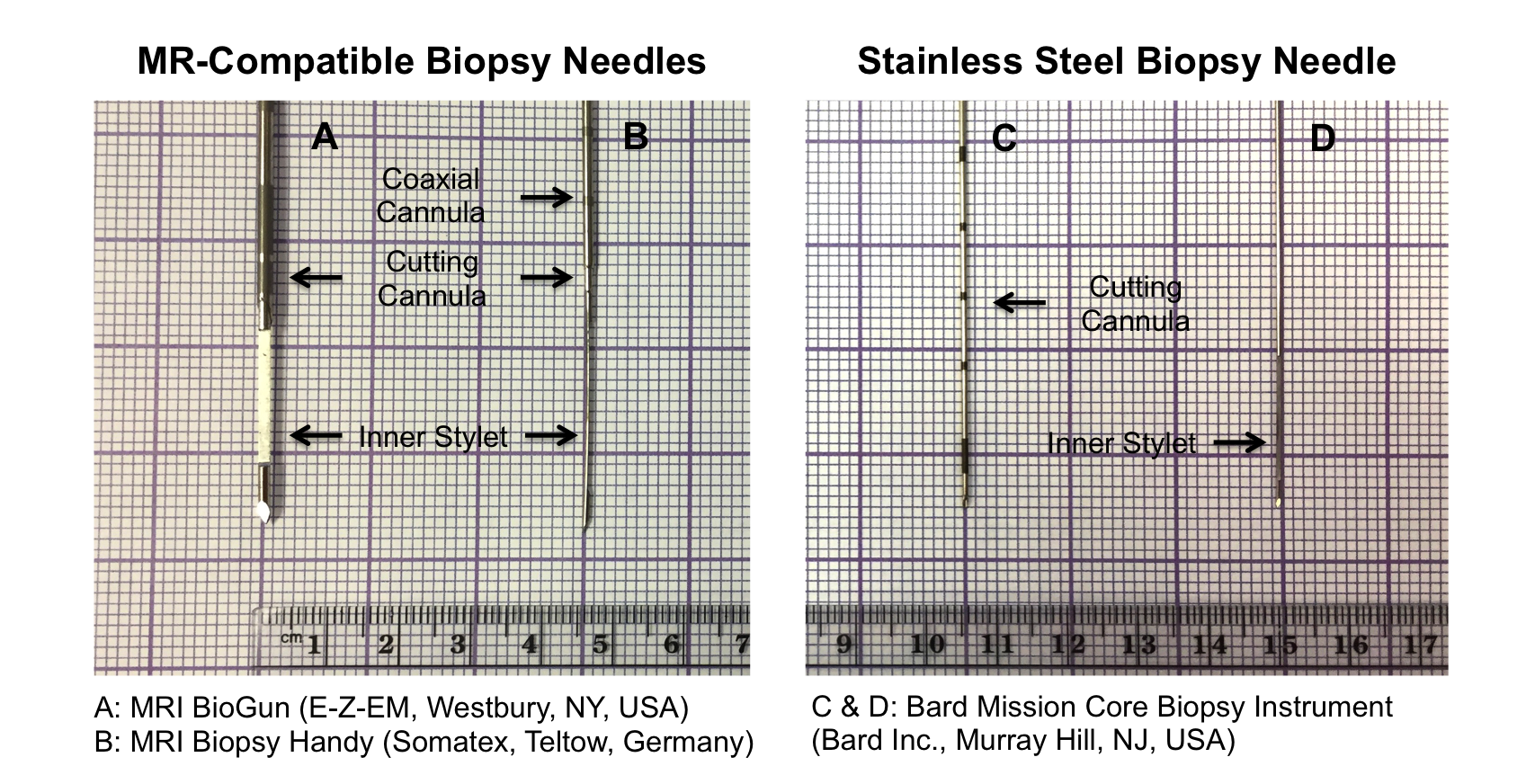
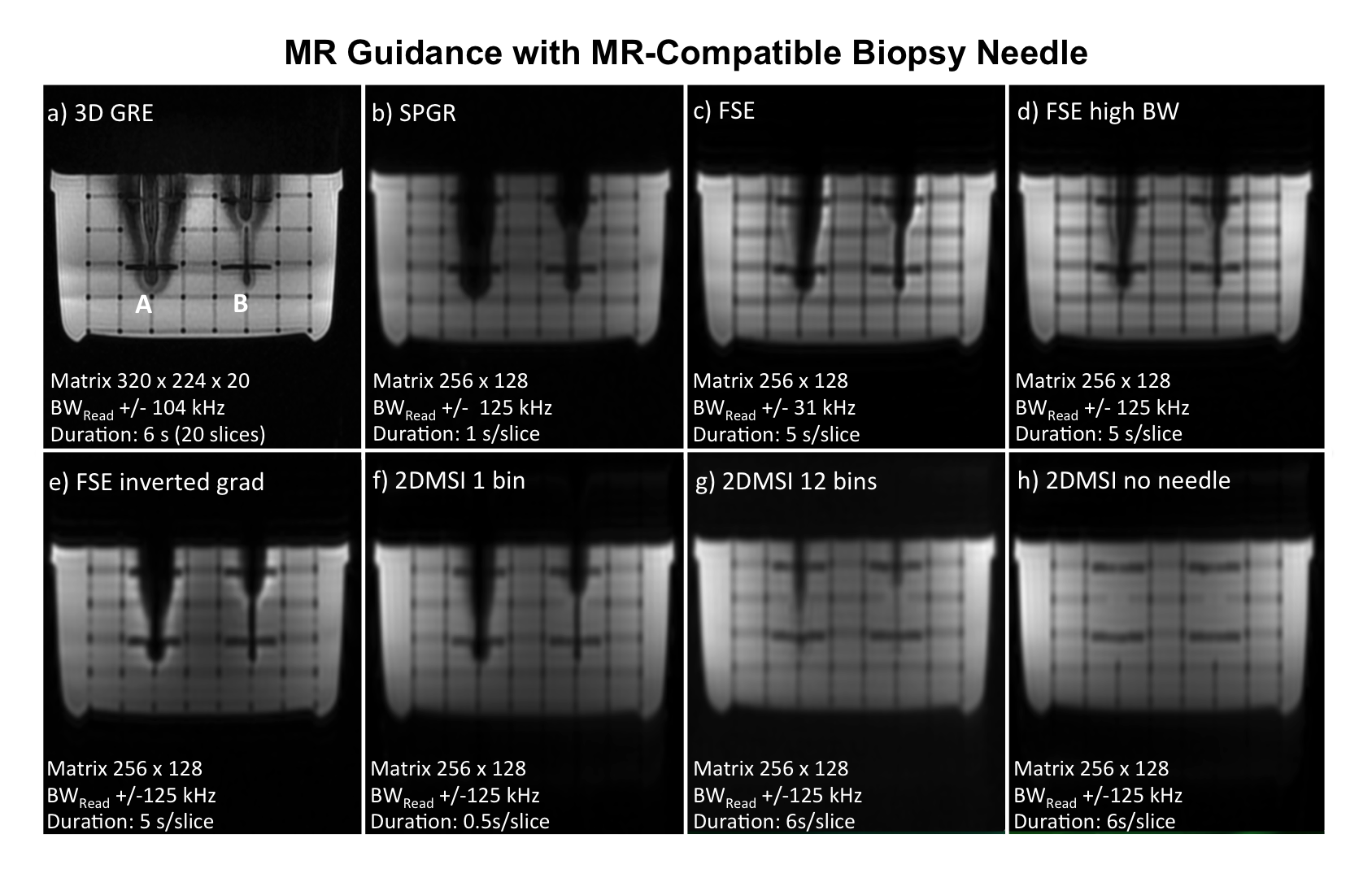
Figure 3: Axial slice containing both MR-compatible biopsy needles, comparing conventional imaging (a & b), alternative artifact reduction techniques (c, d, e) and 2DMSI (f & g). Frame (h) shows the grid phantom without needles as a reference. All images were acquired with FOV 34 cm (cropped), 4 mm slice thickness and the readout oriented in left-right. Whereas the reference techniques suffer from signal void and distortions, 2DMSI with 12 bins also enables artifact-reduced visualization of the off-resonance regions close to the needles and thus more precise needle localization.