2611
Active catheter tracking for MR-Guided Percutaneous Coronary Intervention at 3T: Initial Results in a Pig Model1Department of Radiology, Medical Physics, Medical Center - University of Freiburg, Freiburg, Germany, 2Department of Cardiology and Angiology I, University Heart Center, Freiburg, Germany, 3MaRVis, Frechen, Germany
Synopsis
Compared to X-Ray fluoroscopy, cardiovascular interventions under MR-guidance do not use ionizing radiation, they provide excellent soft tissue contrast, cross-sectional imaging in arbitrary slice orientations and a variety of functional measurement techniques. MR-guided catheterization of coronary arteries has so far only been demonstrated in animal trails at 1.5T, and it remains challenging due to limited temporal and spatial resolution. Also, dedicated instruments for MR-guided coronary interventions are not yet widely available. We show that active visualization of commercial catheters for MR-guided percutaneous coronary in a pig model at 3T is feasible and enables engagement of the LCA under real-time imaging.
Introduction
Compared to X-Ray fluoroscopy, cardiovascular
interventions under MR-guidance do not use ionizing radiation, they provide excellent
soft tissue contrast, cross-sectional imaging in arbitrary slice orientations
and a variety of functional measurement techniques (e.g. blood flow
quantification, perfusion and ventricular function). Over the past years, less
complex MR-guided procedures such as diagnostic right-heart catheterization have
been established and are now performed in studies in humans.1 Catheterization
under MR-guidance of the more complex coronary arteries has so far only been
demonstrated in animal trials at 1.5T, and it remains challenging due to
limited temporal and spatial resolution.2,3 These challenges have
partly been addressed by recent improvements in coronary MRA and real-time
MR-imaging.4,5 In this context, techniques for enhanced catheter and
guidewire visualization (using active or passive tracking6) were
developed to successfully perform the intervention; however, dedicated instruments
for MR-guided coronary interventions are not yet widely available.
In this work, we show initial results of an
MR-guided coronary catheterization in a pig performed at 3T using an active coronary
guiding catheter and MR safe and visible guidewire.Methods
Active Catheter:
The active coronary catheter was constructed from a commercial 5F Tiger catheter (Optitorque, Terumo Medical Corporation). A 2cm-long single-loop coil was attached to the tip of the catheter to allow for localization and visualization of the curvature of the catheter’s distal end. The coil was connected to one receive channel of the MR system via a tuning and matching circuit.
Interventional experiment:
The active catheter was tested in a female minipig (24 months, 41 kg) on a clinical 3T MR system (Siemens PRISMA). After initial sedation, an 8F sheath was placed surgically in the right femoral artery and the animal was brought into the MR system. The animal was mechanically ventilated and general anesthesia was maintained by isoflurane inhalation. For localization of the coronary arteries a whole-heart 3D navigator-gated FLASH sequence with fat saturation and T2 preparation was used (TE/TR: 1.6/3.5 ms, FA: 16°, FoV: 295x295x112 mm³, matrix: 192x192x56 mm, TET2prep: 40 ms, R = 2). From the 3D data, images of the left ostium and main stem were reformatted in both double-oblique transversal (short-axis) and coronal (long-axis) view. These images were then used as references planes for real-time guidance of the active catheter after introduction through the femoral access. Parameters of the real-time radial bSSFP sequence were set to: TE/TR: 1.5/3.0 ms, spokes: 110, FA: 40°, FoV: 280x280x10 mm³, matrix: 192x192, fat saturation. To verify engagement of the left coronary artery (LCA), 3D imaging was repeated and a localized perfusion measurement was performed by injecting 4ml of a 5%-diluted contrast agent solution (ProHance 0.5M, Bracco Imaging) through the catheter. Dynamic contrast enhancement was imaged in five short-axis slices using an ECG-triggered FLASH acquisition with saturation recovery (one shot per slice, 5 slices per heartbeat, TE/TR: 1.1/2.2 ms, TSR: 95 ms, FA: 10°, FoV: 224x290 mm³, matrix: 124x160, R = 2). Finally, a 0.014” MR safe guidewire doped with iron microparticles and providing an additional broader tip marker (MaRVis, Frechen, Germany) was advanced into the left circumflex artery (LCX) during real-time monitoring and the position was verified again with the 3D sequence.
Results
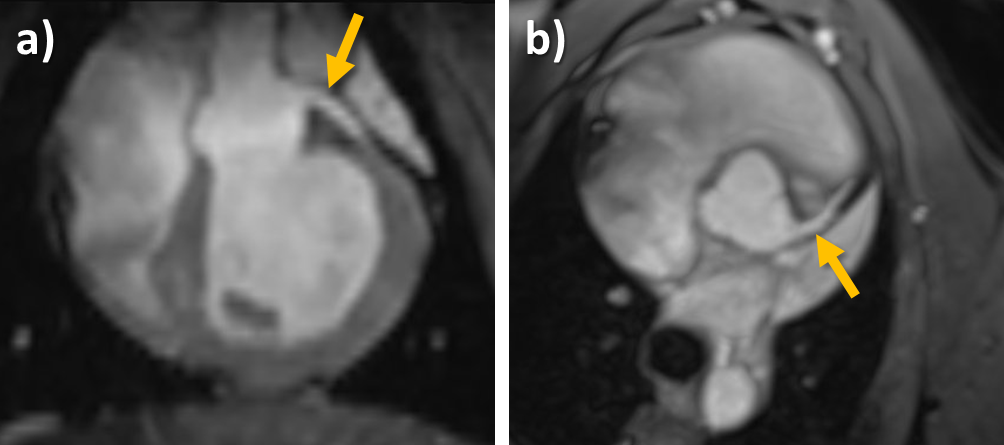
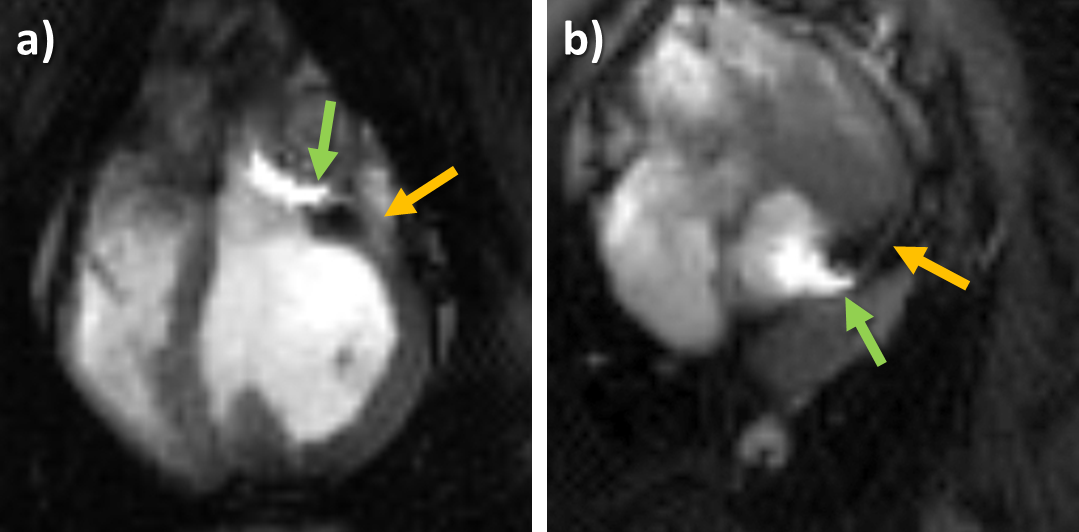
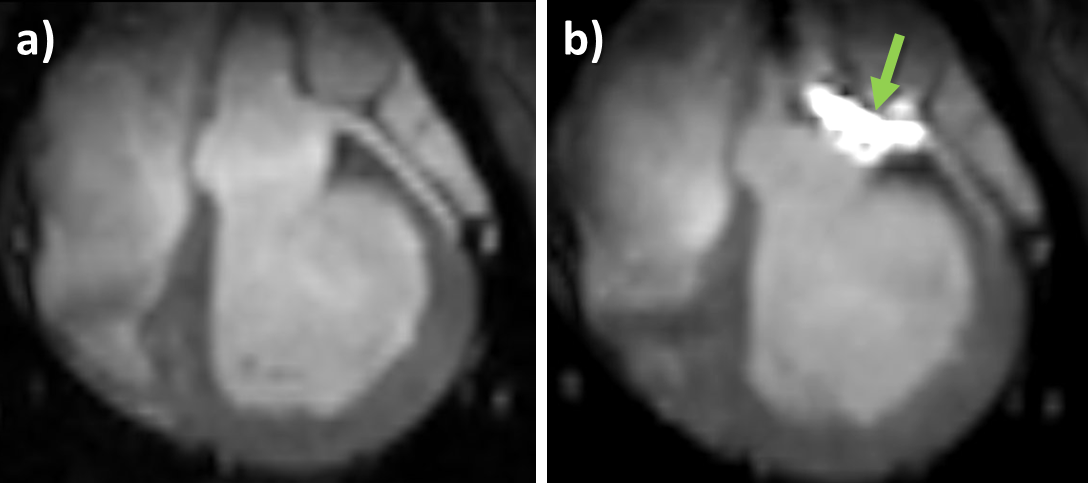
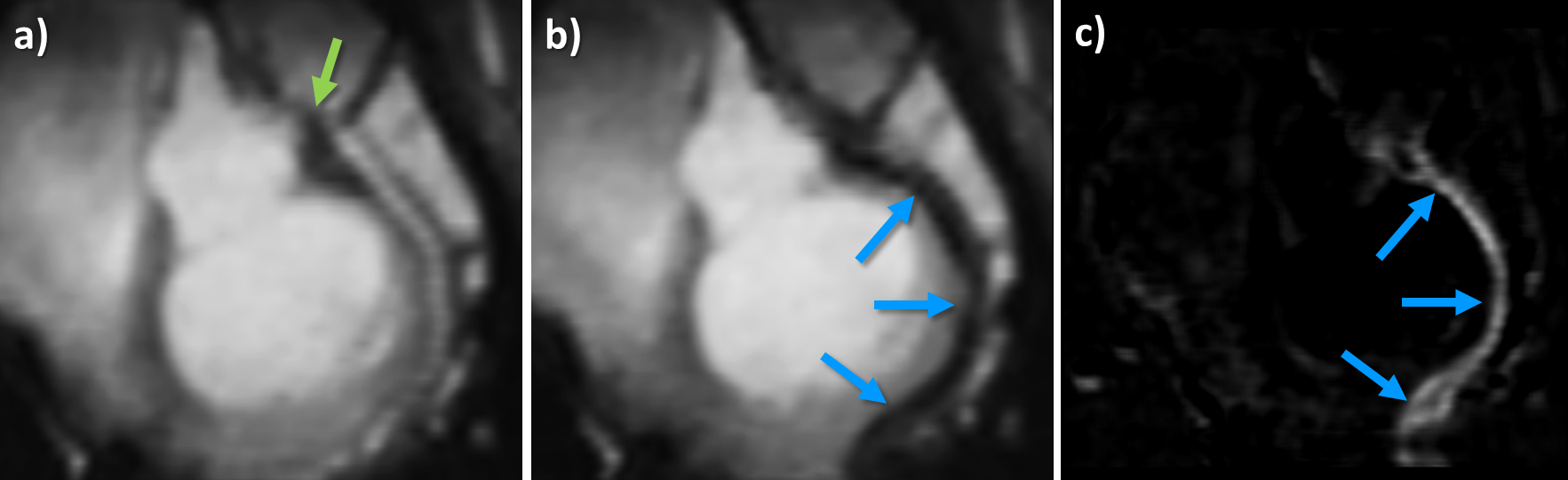
Figure 1 shows reformats of the left coronary main stem acquired before the intervention. Engagement of the artery was successful and could be repeated three times during this experiment. Exemplary real-time images are shown in Figure 2. The tip of the catheter and its curvature are well visible as hyperintense signals together with the left main stem and the proximal part of the LCX. With the catheter in the LCA, 3D images were again acquired (Fig 3) and a localized perfusion measurement was performed (Fig 4). The T1-weighted images clearly depict the myocardial segments supplied via the LCA. Figure 5 shows 3D reformats of the LCX before and after introduction of the guidewire through the catheter. The passive guidewire is clearly detectable by a signal void. The difference image yields a positive contrast of the guidewire which improves delineation especially of the tip marker.Conclusion
We show that active visualization of commercial catheters for MR-guided percutaneous coronary is feasible in a pig model and enables engagement of the LCA under real-time imaging. Although the experiment was done at 3T which is more prone to susceptibility artifacts than 1.5T, bSSFP real-time imaging during the intervention yielded good image quality. Future experiments will also target the right coronary artery and will improve guidewire visualization to perform stent placement at previously defined positions.Acknowledgements
Grant support by the Deutsche Forschungsgemeinschaft (DFG) under grant number BO 3025/2-2 is gratefully acknowledged.
We are thankful to Roland Galmbacher for his help during the animal experiments
References
1. Ratnayaka K, Faranesh AZ, Hansen MS, et al. Real-Time MRI-Guided Right Heart Catheterization in Adults Using Passive Catheters. Eur. Heart J. 2013;34(5):380–389
2. Spuentrup E, Ruebben A, Schaeffter T, et al. Magnetic Resonance–Guided Coronary Artery Stent Placement in a Swine Model. Circulation 2002;105(7):874–879
3. Omary RA., Green JD, Schirf BE. Real-Time Magnetic Resonance Imaging-Guided Coronary Catheterization in Swine. Circulation 2003;107(21):2656–2659.
4. Ginami G, Coppo S, Feng L, et al. Cardiac and Respiratory Motion-Resolved Free-Running Whole-Heart Coronary MRA of Patients Using 5D XD-GRASP Reconstruction. Proc. Intl. Soc. Mag. Reson. Med. 2016
5. Zhang S, Uecker M, Voit D, et al. Real-Time Cardiovascular Magnetic Resonance at High Temporal Resolution: Radial FLASH with Nonlinear Inverse Reconstruction. J. Cardiov. Magn. Reson. 2010;12:39
6. Bock M, Wacker FK. MR-Guided Intravascular Interventions: Techniques and Applications. J. of Magn. Reson. Imaging 2008; 27(2):326–338
Figures