2609
Visualization of Intracranial Aneurysms Treated with Low-profile Visualized Intraluminal Support (LVIS Jr. stent) Using Ultrashort Echo Time Magnetic Resonance Angiography1Department of Radiology, Graduate School of Medicine, Juntendo University, Tokyo, Japan, 2Department of Radiology, Juntendo University Hospital, Tokyo, Japan, 3Department of Neurosurgery, Juntendo University School of Medicine, Tokyo, Japan, 4Department of Neuroendovascular Therapy, Juntendo University School of Medicine, Tokyo, Japan
Synopsis
In this study, we evaluated the usefulness of ultrashort echo time magnetic resonance angiography (Silent MRA) for intracranial aneurysms treated with LVIS Jr. stent-assisted coil embolization by a comparison between silent MRA and three-dimensional time of flight MRA (3D TOF-MRA) because the LVIS Jr. stent had higher metal coverage than previous reported stents. In silent MRA, the score of flow in the stents was superior to that of 3D TOF-MRA (p<0.05). Moreover, aneurysm occlusion status was good agreement for DSA. Therefore, silent MRA might be useful for intracranial aneurysms treated with LVIS Jr. stent-assisted coil embolization.
Background and Purpose
Follow-up of intracranial aneurysms treated with intracranial stent using three-dimensional time of flight MRA (3D TOF-MRA) is difficult to visualize flow in an intracranial stent due to susceptibility artifacts produced by metallic devices.1 The LVIS Jr. stent is a self-expandable single wire braided stent with 1.5 mm cells. The LVIS Jr. stent has three radiopaque tantalum markers on the proximal and distal tines with three tantalum helical strands within the stent body.2,3 This stent design is higher metal coverage than previous reported stents.4 Therefore, we should assess the stent related magnetic susceptibility. In magnetic resonance imaging, short echo time can reduce the phase dispersion of the blood flow signal and decreases artifacts of magnetic susceptibility. Thus, UTE may depict an in stent flow. The purpose of this study was to assess the usefulness of non-contrast enhanced MRA using ultrashort echo time acquisition (silent MRA) for intracranial aneurysms treated with LVIS Jr. stent-assisted coil embolization by a comparison between silent MRA and 3D TOF-MRA.Methods
Thirty one aneurysms treated with LVIS Jr. stent underwent silent MRA, 3D TOF-MRA, and DSA. Two neuroradiologists independently reviewed the MRA images and subjectively scored the flow in the stents on a scale of 1 (not visible) to 4 (excellent). We evaluated the aneurysm occlusion status using the two grade scale (total occlusion and neck or aneurysm remnant). Interobserver and intermodality agreement were analyzed by weighted kappa statistics. Using consensual X-ray DSA as a reference standard to evaluate the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated for both MRAs.Results
The average score ± standard deviation for silent MRA was 3.16 ± 0.79 and 1.48 ± 0.67 (p < 0.05) for 3D TOF-MRA. Interobserver agreement was substantial agreement (κ=0.66). The rate of two grade scale were 69% and 31% for DSA, 65% and 35% for silent MRA, and 92% and 8% for 3D TOF-MRA, respectively. Intermodality agreement was 0.88 for DSA/Silent MRA and 0.30 for DSA/3D TOF-MRA, respectively. The sensitivity, specificity, and positive and negative predictive values of the silent MRA relative to DSA were 100%, 93%, 89%, and 100%, respectively. For 3D TOF-MRA relative to DSA, sensitivity, specificity, and positive and negative predictive values were 26%, 100%, 100%, and 75%.Discussion
Silent MRA uses an ultrashort echo time (UTE) combined with arterial spin labeling (ASL).5 ASL technique is used as a preparation pulse for visualization of the blood flow and data acquisition is based on 3D radial sampling.5,6 Though LVIS Jr. stent had higher metal coverage, silent MRA was able to depict an in stent flow. UTE minimizes phase dispersion of signal of the labeled blood flow and decreases susceptibility artifacts to metallic device. Therefore, silent MRA could visualize precisely than 3D TOF-MRA. In silent MRA, aneurysm occlusion status was good agreement for DSA. The silent MRA has possibility to replace DSA at follow-up of intracranial aneurysms treated with intracranial stents.Conclusion
Ultrashort echo time MRA (Silent MRA) might be useful for follow-up of intracranial aneurysms treated with LVIS Jr. stent-assisted coil embolization.Acknowledgements
This work was funded by ImPACT Program of Council forScience, Technology and Innovation (Cabinet Office, Government ofJapan).
This work is supported by a Grant-in-Aid for Scientific Research onInnovative Areas (ABiS) from the Ministry of Education, Culture,Sports, Science and Technology of Japan.
References
1 Kovacs A, Möhlenbruch M, Hadizadeh DR, et al. Noninvasive imaging after stent-assisted coiling of intracranial aneurysms: comparison of 3-T magnetic resonance imaging and 64-row multidetector computed tomography: a pilot study. J Comput Assist Tomogr. 2011;35:573–582
2 Behme D, Weber A, Kowoll A, et al. Low-profile Visualized Intraluminal Support device (LVIS Jr) as a novel tool in the treatment of wide-necked intracranial aneurysms: initial experience in 32 cases. J Neurointerv Surg. 2015;7(4):281-5
3 Ge H, LV X, Yang X, et al. LVIS Stent Versus Enterprise Stent for the Treatment of Unruptured Intracranial Aneurysms. World Neurosurg. 2016;91:365-70
4 Spiotta AM, Miranpuri A, Chaudry MI, et al. Combined balloon stent technique with the Scepter C balloon and low-profile visualized intraluminal stent for the treatment of intracranial aneurysms. J Neurointerv Surg. 2013;5 Suppl 3:iii79-iii82
5 Irie R, Suzuki M, Yamamoto M, et al. Assessing Blood Flow in an Intracranial Stent:A Feasibility Study of MR Angiography Using a Silent Scan after Stent-Assisted Coil Embolization for Anterior Circulation Aneurysms. AJNR Am J Neuroradiol. 2015;36:967-70
6 Alibek S, Vogel M, Sun W, et al. Acoustic noise reduction in MRI using Silent Scan: an initial experience. Diagn Interv Radiol. 2014;20:360-3
Figures
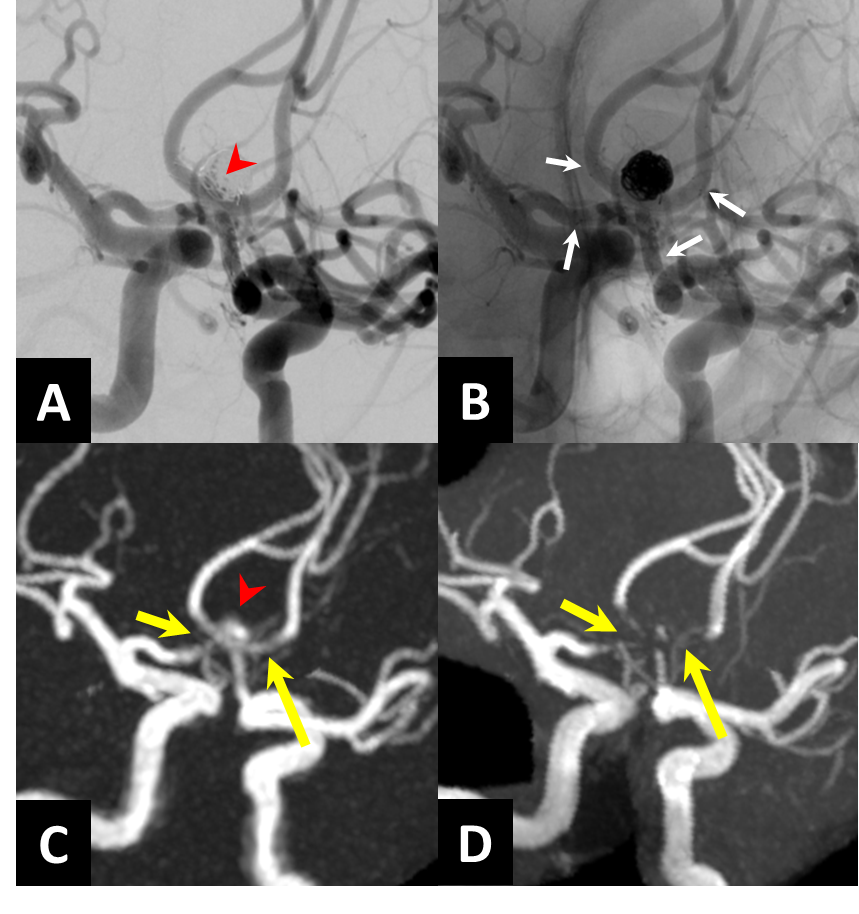
Fig.1
A. X-configuration stent-assisted coil embolization is performed with LVIS Jr. stents. (Red arrow head shows neck remnant.)
B. X -ray digital angiography (White arrows are stent edges.)
C. Silent MRA shows minimal signal loss at stented segments (yellow arrows). Neck remnant is depicted clearly (red arrow head).
D. 3D TOF-MRA shows almost signal loss at stented segments (yellow arrows). The depiction of neck remnant is difficult.
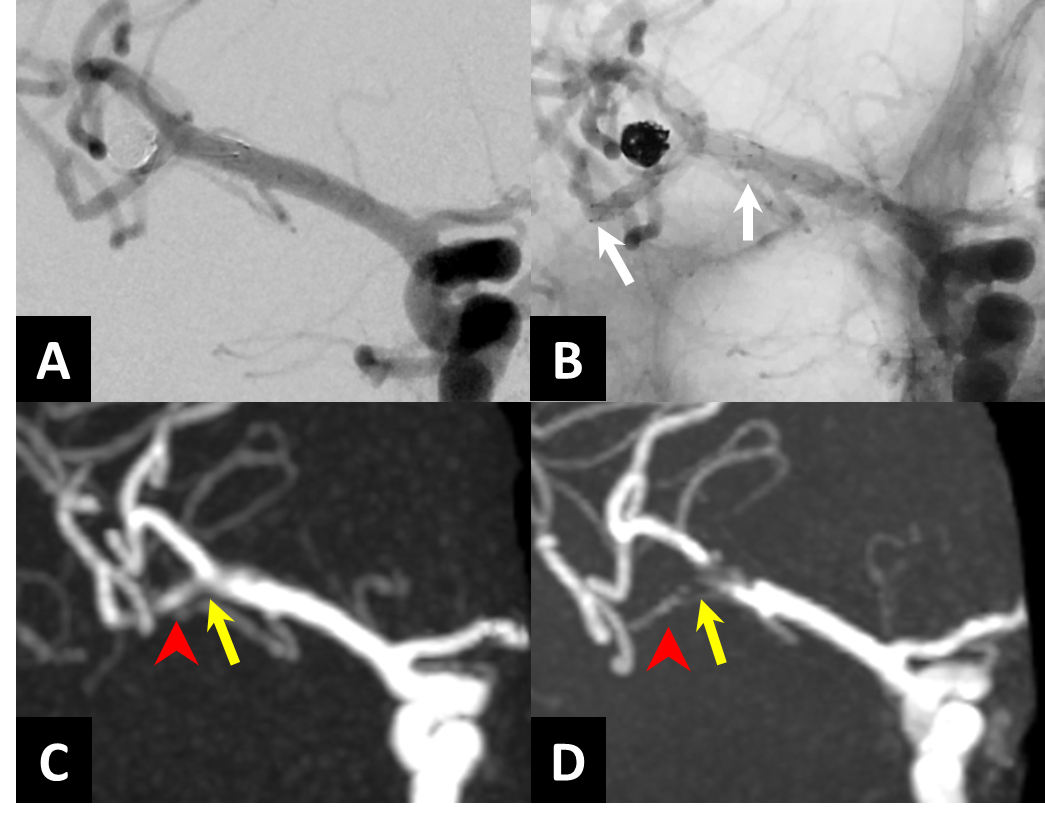
Fig.2
A. Stent-assisted coil embolization is performed with LVIS Jr. stent for Rt.MCA. X -ray digital subtraction angiography shows complete occlusion.
B. X -ray digital angiography (White arrows are stent edges.)
C. Silent MRA shows minimal signal loss at stented segment (yellow arrow). The in-stent stenosis is not suspected (red arrow head). It is true negative.
D. 3D TOF-MRA shows strong signal loss at stented segment of Rt.MCA bifurcation (yellow arrow). Distal of Rt.MCA suspects the in-stent stenosis (red arrow head). However, it is false positive.