2559
High-resolution spinal DTI imaging using RESOLVE sequence in multiple sclerosis and clinical isolated syndromeNingnannan Zhang1, Zhang Zhang1, Tianyi Qian2, Wen Qin1, Qiuhui Wang1, and Chunshui Yu1
1Department of Radiology, Tianjin Key Laboratory of Functional Imaging, Tianjin Medical University General Hospital, Tianjin, People's Republic of China, 2MR Collaborations NE Asia, Siemens Healthcare, Beijing, People's Republic of China
Synopsis
This study reports the preliminary application of high-resolution diffusion tensor imaging (DTI) using readout segmentation of long variable echo trains (RESOLVE) sequence for spinal cord imaging in patients with demyelinating conditions. Patients with clinical isolated syndrome (CIS) and multiple sclerosis (MS) were recruited in order to investigate image evidences in early stages and the progression of the disease. The results of DTI analyses demonstrate that MS is characterized by diffuse axonal compensation in the spinal cord.
PURPOSE
The spinal cord is a common site of pathology in multiple sclerosis (MS) and clinical isolated syndrome (CIS). Diffusion-weighted MRI (DWI) techniques show promise in the evaluation of pathological states of the spine, and in the detection of occult damages in normal appearing tissues of the spinal cord. Traditional single-shot echo planar imaging (EPI) - based DWI is limited by the acquisition of axial images only and is susceptible to artifacts that manifest as geometric distortion, signal drop, and image blurring. The diffusion tensor imaging (DTI) technique is challenging for spinal cord imaging due to the small area of the cord, cardiac and respiratory motion artifacts. The readout segmentation of long variable echo trains (RESOLVE) sequence permits the use of extremely short echo spacing, independent of the spatial resolution, thereby reducing image distortions and allowing for large range spinal cord scans in the sagittal view. In this study, we performed high-resolution DTI using the RESOLVE sequence to explore the disease damage pattern of the cervical spinal cord with MS and CIS.METHODS
Nine MS patients and seven age- and gender-matched CIS patients were recruited for this study. All MRI scans were performed on a MAGNETOM Skyra 3T MR scanner (Siemens, Erlangen, Germany). Conventional sequences (axial and sagittal T2WI/T1WI, fat-suppressed sagittal T2WI) and a high-resolution RESOLVE1 sequence with DTI mode were applied. Imaging parameters were: iPAT factor = 2 (GRAPPA); field of view = 220mm; TR/TE = 2000/53 ms; matrix = 110×100; slice thickness = 2.0mm; number of readout segment = 5; diffusion directions = 20; b-values = 0 and 1000s/mm2; total scan time = 4 minutes 20 seconds. The regions of interest (ROIs) of each segmental cervical level were defined manually (Figure 1). The mean values of fractional anisotropy (FA), mean diffusivity (MD), three eigenvalues (λ1, λ2, λ3), radial diffusivity (RD, RD = [λ2+λ3]/2), and axial diffusivity (AD, AD = λ1) were generated. Independent-sample t-test was used to compare the differences between two groups at the level of the lesion, the preserved sites, and all sites of the spinal cord.RESULTS
No significant tensor index differences (MD and AD) were found in lesion sites between MS and CIS patients (Figure 2). Compared to CIS, the RD of MS was significantly reduced at the preserved sites (RD: 0.507×10-3 vs. 0.614×10-3, p = 0.050), and at all sites (RD: 0.514×10-3 vs. 0.524×10-3, p = 0.041), while FA was increased at all sites (0.672 vs. 0.594, p = 0.021) (Figure 2).DISCUSSION
DTI of the spinal cord is challenging, because of its low resolution, especially in the sagittal view. RESOLVE enables high-resolution DTI by minimizing distortions and T2* blurring. The decreased RD and therefore higher FA in MS suggested an increased axonal density or decreased axonal diameter. These axonal changes were visualized in both preserved and all sites of the cervical spinal cord. This supported the current understanding that MS is a diffuse disease process and that a compensatory mechanism during the disease progression may exist.CONCLUSION
High-resolution spinal DTI using the RESOLVE sequence is feasible in the clinical study of the spinal cord. The images in our study implied a different spinal cord damage pattern in MS compared to CIS patients.Acknowledgements
This work was supported by the Tianjin Key Technology R&D Program (14ZCZDSY00018).References
1. Porter DA et al. High resolution diffusion - weighted imaging using readout-segmented echo-planar imaging, parallel imaging and a two - dimensional navigator - based reacquisition. Magn Reson Med. 2009;62: 468-475.Figures
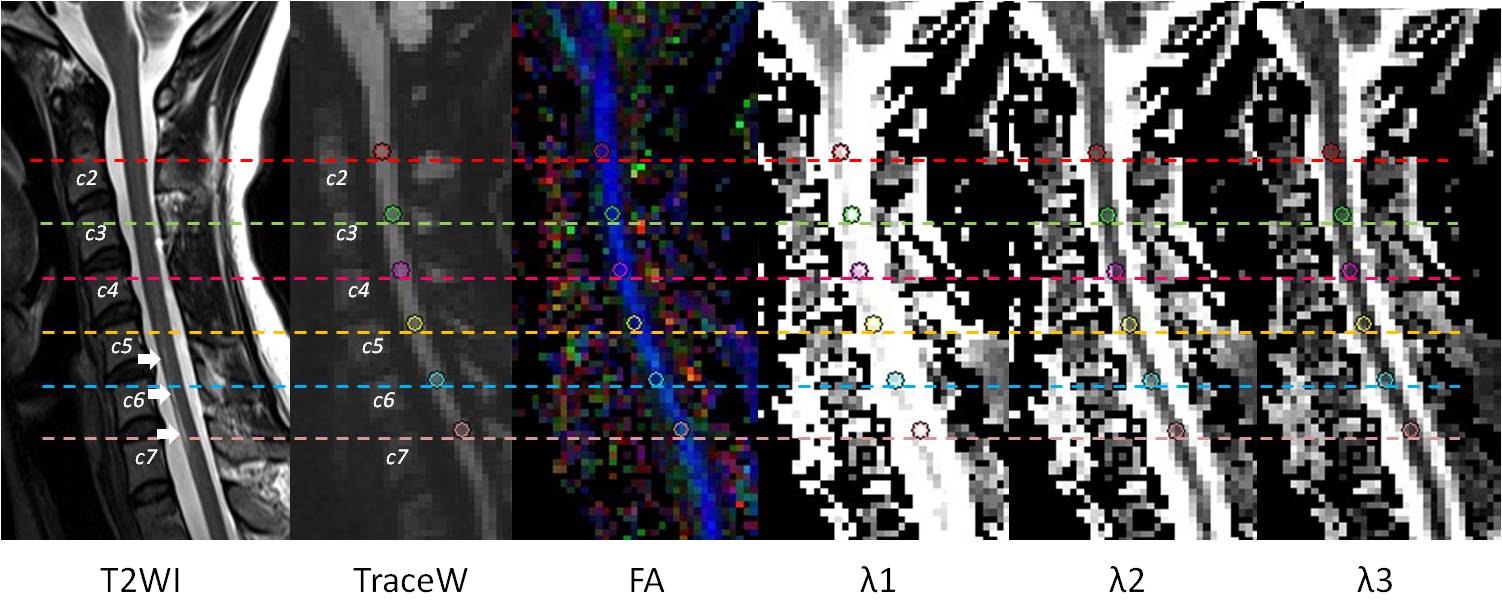
Figure 1. ROI
examples in the cervical spinal cord of a CIS patient. Hyperintense zones
related to the lesion are seen at levels C5, C6 and C7 of the T2-weighted image
(white arrow). The ROIs are plotted on the sagittal images of TraceW, FA and
three eigenvalues (λ1, λ2, λ3) maps at each level (C2 - C7).
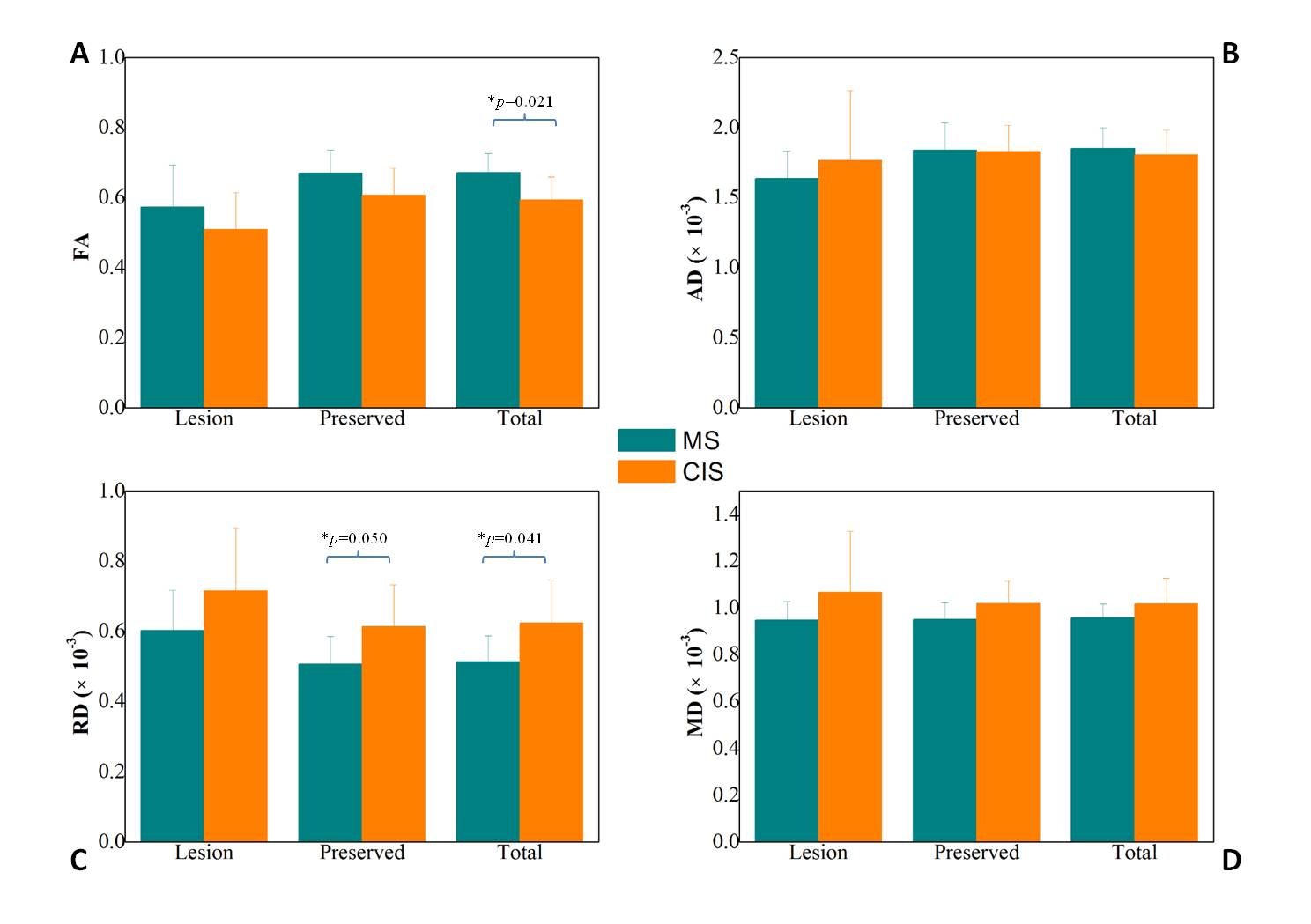
Figure 2. DTI index comparison between MS and
CIS in different sites. FA of MS was significantly higher than CIS at all sites
(0.672 vs. 0.594, p=0.021), but there was no significant difference at the
other two sites (p>0.05) (Figure 2A). The RD of MS was significantly lower
than in CIS at both preserved sites (RD: 0.507×10-3 vs. 0.614×10-3,
p=0.050), and all sites (RD: 0.514×10-3 vs.
0.524×10-3,
p=0.041), but there was no significant difference at lesion sites (Figure 2C).
No significant DTI index differences were found between MS and CIS patients for
AD and MD (p>0.05) (Figure 2B and 2D).