2551
Baseline DTI discriminates and predicts MS from ADEM1Washington University in St. Louis, School of Medicine, St. Louis, MO, United States, 2St. Louis University, School of Medicine, St. Louis, MO, United States
Synopsis
MS is a progressive disorder in which demyelination, axonal degeneration, and inflammation contribute to disease pathogenesis. ADEM is classically an acute, monophasic demyelinating disease in which axonal damage is present but minimal. About 20 percent of ADEM cases can have relapses and are diagnosed with MS later, posing a diagnostic dilemma at initial presentation. In this study, we investigate the role of directional diffusivity DTI as a MR biomarker to differentiate and predict Acute Disseminated Encephalomyelitis (ADEM) from Multiple Sclerosis (MS) in pediatric patients.
Objective:
To investigate the role of directional diffusivity measures from Diffusion Tensor Imaging (DTI) as a MR biomarker to differentiate Acute Disseminated Encephalomyelitis (ADEM) from Multiple Sclerosis (MS) in pediatric patients.Introduction:
MS is a progressive disorder in which demyelination, axonal degeneration, and inflammation contribute to disease pathogenesis. ADEM is classically an acute, monophasic demyelinating disease in which axonal damage is present but minimal.1, 2 About 20 percent of ADEM cases can have relapses and are diagnosed with MS later, posing a diagnostic dilemma at initial presentation. DTI directional diffusivity, a quantitative MR technique, may be useful to predict the development of MS at the first attack of demyelination. 3,4Methods:
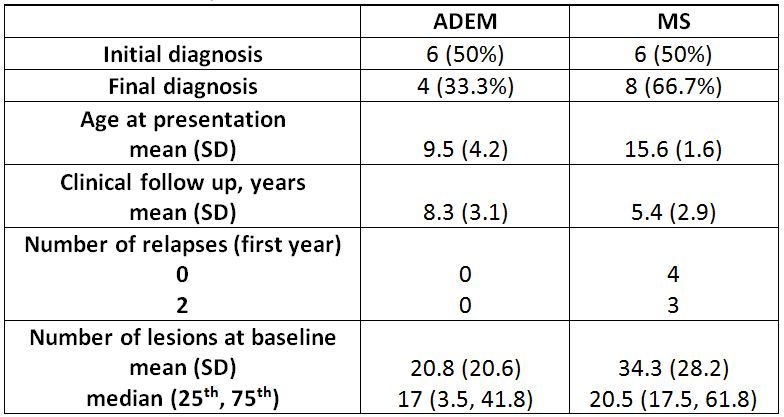
Twelve patients with acute demyelination, 6 with encephalopathy (initial diagnosis of ADEM) and 6 without encephalopathy (initial diagnosis of clinically isolated syndrome with high risk for MS) had standard clinical MR protocol with additional DTI. The DTI scans were performed within 12 months from the date of clinical presentation. Patients were followed for an average of 6.8 years. Six patients with clinically isolated syndrome and 2 patients with ADEM were diagnosed with MS after having relapses without encephalopathy. Control subjects consist of age-matched healthy individuals for each patient. Demographics are summarized in Table 1.
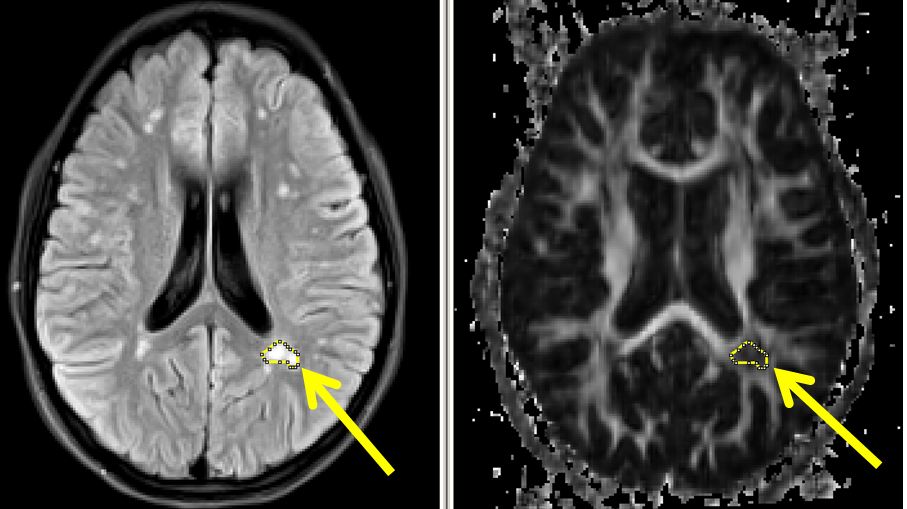
DTI scans were processed off-line using in-house program to obtain directional diffusivity maps consisting of fractional anisotropy (FA), mean diffusivity, axial diffusivity, and radial diffusivity. The images were registered to age matched atlas space of 1*1*1. Region of interest (ROI) drawn based on hyperintensity abnormality on FLAIR image of subject using ImageJ (shown in Figure 1) with the following selection criteria a) the lesion must appear in at least five continuous slices, and b) ROI selectedonly once in the highest hyperintensity slice.
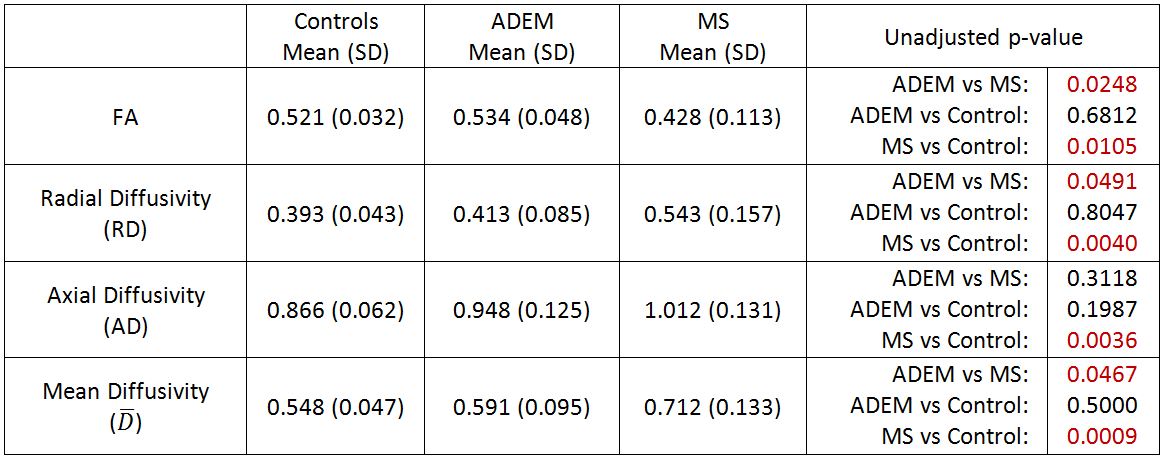
Statistical Analysis: Descriptive statistics were used to summarize demographic and clinical characteristics (mean (SD) or frequencies (%n), Table 1). Mixed models using restricted maximum likelihood estimation controlling for the repeated measures within each subject were used to identify differences in DTI measures (FA, axial, radial and mean diffusivity) between patients with ADEM, MS, and controls (shown in Table 2).
Results:
DTI ROI analysis revealed differences in white matter microstructural characteristics between MS and ADEM patients at the baseline. Significant differences for FA map (ADEM vs MS p<0.03) and RD map (ADEM vs MS p<0.05) were observed, this difference did not persist after post-hoc adjustment. Lower FA values and higher AD and RD values in MS patients indicate possible demyelination or axonal damage consistent with MS pathologic features. These preliminary results suggest that DTI directional diffusivity measures FA and RD may have the potential to serve as biomarkers for distinguishing ADEM from MS and may play an important role as outcome measures in neuroprotective and reparative studies. Further studies with more patients are needed.Acknowledgements
This work was supported by National Multiple Sclerosis Society grants RG 4190A2/1, and PP1361.References
1. Di Bari M, Di Pinto G, Reale M, Mengod G, Tata AM., “Cholinergic system and neuroinflammation: Implication in multiple sclerosis”, Cent Nerv Syst Agents Med Chem. 2016 Aug 22. PMID: 27550615
2. Dale RC, de Sousa C, Chong WK, Cox TC, Harding B, Neville BG., “Acute disseminated encephalomyelitis, multiphasic disseminated encephalomyelitis and multiple sclerosis in children”, Brain, 2000 Dec;123 Pt 12:2407-22. PMID: 11099444
3. Hintzen RQ, Dale RC, Neuteboom RF, Mar S, Banwell B.” Pediatric acquired CNS demyelinating syndromes: Features associated with multiple sclerosis.” Neurology, 2016 Aug 30;87(9 Suppl 2):S67-73. doi: 10.1212/WNL.0000000000002881. PMID: 27572864
4. Vishwas MS, Healy BC, Pienaar R, Gorman MP, Grant PE, Chitnis T., “Diffusion tensor analysis of pediatric multiple sclerosis and clinically isolated syndromes”, AJNR Am J Neuroradiol. 2013 Feb;34(2):417-23. doi: 10.3174/ajnr.A3216. PMID: 22859275
Figures