2532
Assessment of neuronal dysfunction in benign multiple sclerosis: a sodium MRI study1Aix-Marseille Univ, CNRS, CRMBM, Marseille, France, 2Aix-Marseille Univ, APHM, Hopital de la Timone, CEMEREM, Marseille, France, 3Aix Marseille Univ, APHM, Hôpital de la Timone, Pôle de Neurosciences Cliniques, Service de Neurologie, Marseille, France
Synopsis
Assessment of neuro-degenerative process in multiple sclerosis using sodium MRI. A study in a population of 135 subjects at different disability and disease duration
Background
The natural course of multiple sclerosis (MS) is highly variable between patients. Some of them are particularly notable by a relative small number of relapses followed by a good recovery and subsequently a lower disability after a long disease course (so-called benign MS-BMS). Nevertheless, this low level of disability is not explained by T2 lesion load, which can be high even if the patient had a benign evolution. To explain this paradox, we can hypothesize that this relative “better” evolution is related to a less irreversible neurodegenerative process compared to patient with a more “classical” MS evolution. Recent studies have evidenced in vivo brain sodium accumulation in MS from the earliest stage to the progressive forms [1]–[5]. All these studies suggest that sodium accumulation is related to ionic exchanges dysfunction known to lead to irreversible neuro-axonal loss in MS. Thus, we can hypothesize that BMS patients are relatively spared from sodium accumulation, and consequently from neuronal injury, than relapsing remitting MS (RRMS) patients having the same disease duration. Nevertheless, because BMS patients can develop secondary progressive MS and because we previously showed that sodium accumulation increases with disease duration [2], we can also hypothesize that BMS patients are more affected than early RRMS even if they have the same level of disability.Objective
To assess neuro-degenerative process in benign multiple sclerosis (BMS) and to assess the link between sodium accumulation, disability and disease duration.Methods
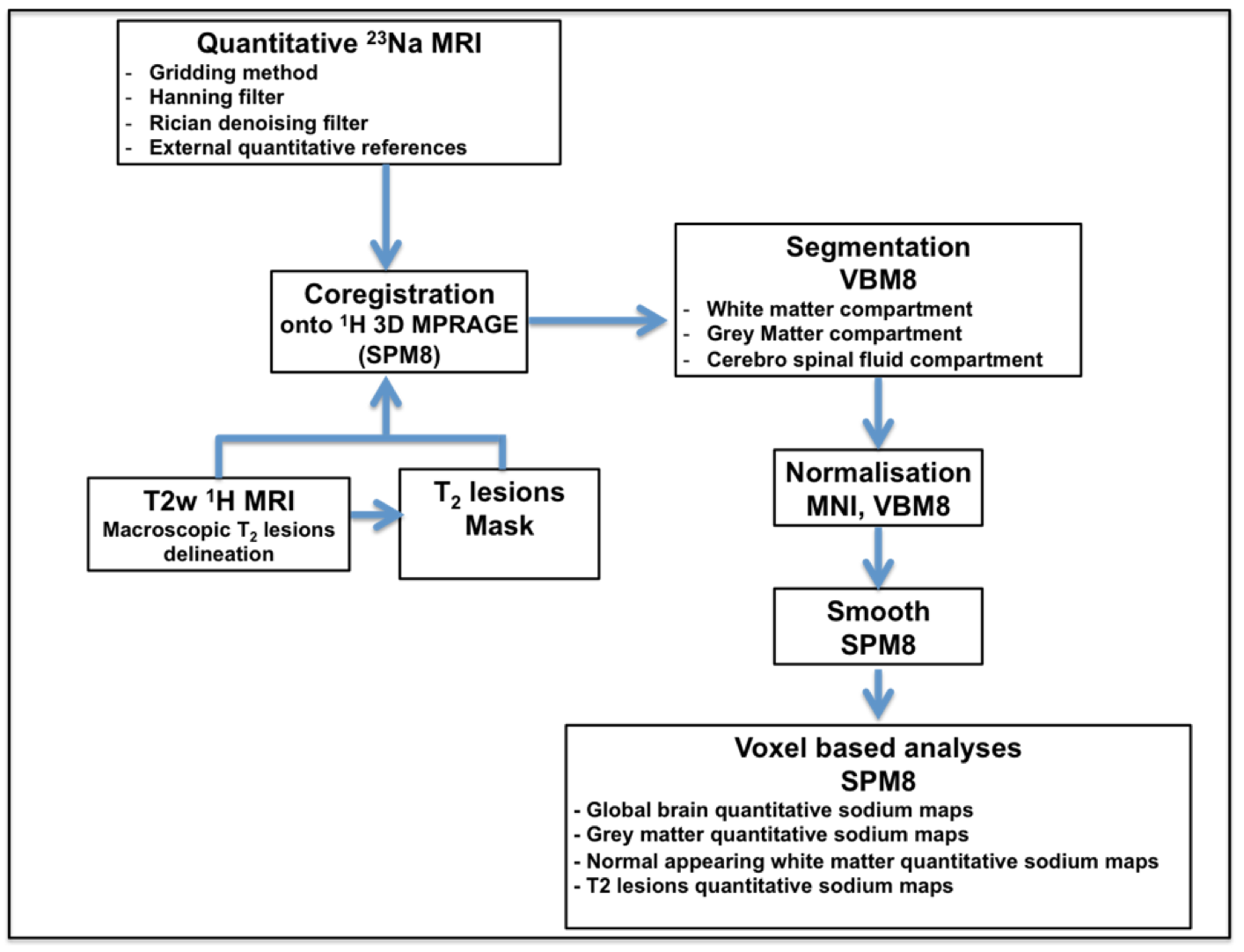
135 subjects were enrolled in the study (n=21 BMS patients with a disease duration ≥ 15 years, without any drugs and EDSS (scale of disability) < 3.0; n=25 “late” RRMS patients with same disease duration as BMS; n=33 “early” RRMS with same EDSS as BMS but with a mean disease duration of 1.6 years; and n=56 age and sex matched controls). MRI exams were performed at 3T (Verio, Siemens). 23Na MRI was acquired using a double-tuned 23Na-1H volume head coil (RapidBiomedical) and a 3D density-adapted radial projection reconstruction pulse sequence (TE=200μs/TR=120ms, 17000 projections and 369 samples per projection, 3.6mm3 isotropic resolution, acquisition time = 34min) with two tubes filled with 50 mM of sodium placed in the FOV to serve for external references. High-resolution proton MRI 3D-MPRAGE (TR=2300ms/TE=3ms/TI=900ms, 160 slices, 1mm3 isotropic resolution) was obtained using a 32-element 1H head coil (Siemens). The optimized post-processing pipeline is described in Figure 1. A voxel-based statistical mapping analysis (SPM8) was conducted onto the spatially normalized and smoothed quantitative sodium concentration maps of all subjects to compare at the voxelwise level the total sodium concentration (TSC) between MS patients and healthy controls (SPM8, p<0.005, FDR corrected). Comparisons of TSC in white matter (WM) and grey matter (GM) compartment between patients and controls were assessed using t-test, considered significant for a p ≤ 0.05.Results
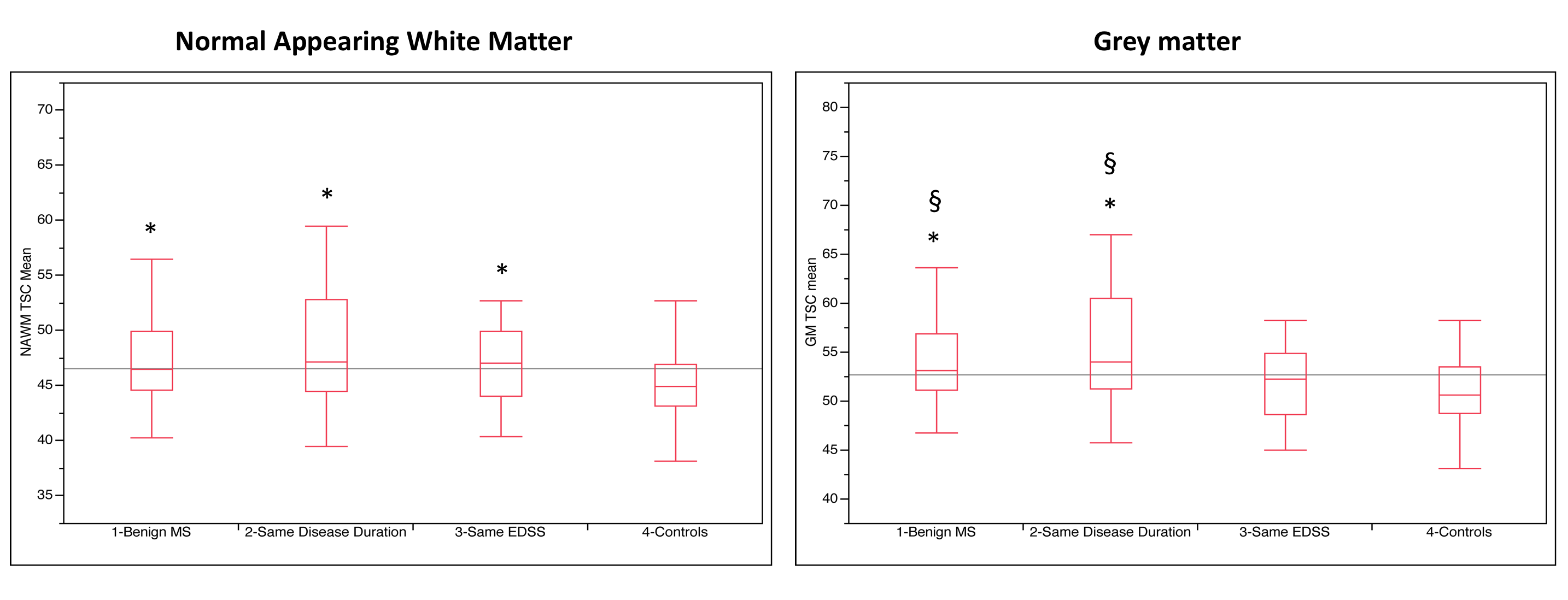
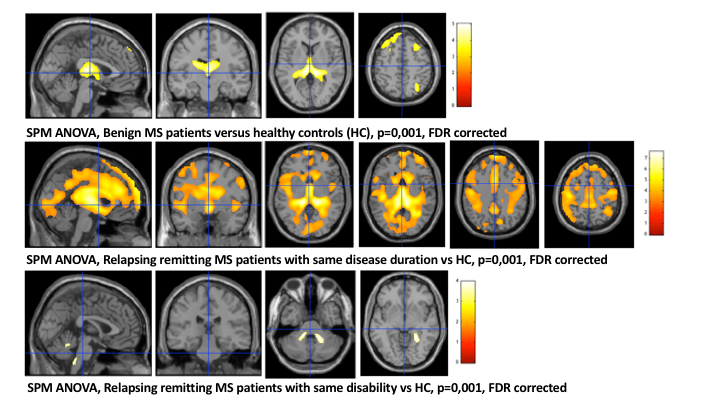
The mean disease duration of BMS patients was 19.2 years (SD=5.4) and the median EDSS was 1.5 [Range= 0-2.5]. The mean disease duration of “late” RRMS patients was 19.0 years (SD=7.7) with a median EDSS of 4 [Range= 2-7.5]. Finally, the mean disease duration of “early” RRMS patients was 1.6 years (SD=0.2) with a median EDSS of 1 [Range= 0-2.5]. TSC was significantly increased (p<0.05) in normal appearing white matter (NAWM) and GM in BMS and RRMS with same disease duration compared to controls (Figure 2). TSC was significantly increased (p<0.05) also in GM of BMS and RRMS with same disease duration compared to RRMS with same disability but lower disease duration. Statistical mapping analysis showed that this sodium accumulation was located bilaterally in the thalami, the cerebellum and the right supramarginal gyrus for BMS patients compared to controls. As expected, this sodium accumulation was more widespread for RRMS patients with same disease duration while this sodium accumulation was very restricted in early RRMS patients despite the same level of disability (Figure 3).Conclusion
This study demonstrates that BMS patients are affected by sodium accumulation that could be related to neuro-degeneration. This accumulation seems to be less pronounced in BMS than in patients with a same disease duration but with a higher disability but more pronounced than in early stage of the disease even if the disability is similar, suggesting that sodium accumulation and consequently neuro-degeneration can be related to the combination of the disability in a main part and the disease duration in a lower part. Future longitudinal studies are needed to evaluate the precise impact of sodium accumulation on disability compared to disease duration.Acknowledgements
No acknowledgement found.References
1. Inglese M, Madelin G, Oesingmann N, et al. Brain tissue sodium concentration in multiple sclerosis: a sodium imaging study at 3 tesla. Brain. 2010; 133(3):847–857.
2. Zaaraoui W, Konstandin S, Audoin B, et al. Distribution of brain sodium accumulation correlates with disability in multiple sclerosis: a cross-sectional 23Na MR imaging study. Radiology. 2012; 264(3):859–867.
3. Paling D, Solanky BS, Riemer F, et al. Sodium accumulation is associated with disability and a progressive course in multiple sclerosis. Brain. 2013; 136(7):2305–2317.
4. Maarouf A, Audoin B, Konstandin S, et al. Topography of brain sodium accumulation in progressive multiple sclerosis. Magma N. Y. N. 2014; 27(1):53–62.
5. Petracca M, Vancea RO, Fleysher L, et al. Brain intra-and extracellular sodium concentration in multiple sclerosis: a 7 T MRI study. Brain. 2016:awv386.
Figures