Chinese National Natural Science Foundation
2527
Iron is a biomarker for differentiating multiple sclerosis lesions from ischemic demyelinating lesionsWeiwei Chen1, Yan Zhang1, Ketao Mu1, Susan A. Gauthier2, Yi Wang3,4, and Wenzhen Zhu1
1Tongji hospital, Tongji Medical College, Huazhong University of Science & Technology, Wuhan, People's Republic of China, 2Neurology, Weill Cornell Medical College, NY, United States, 3Radiology, Weill Cornell Medical College, NY, United States, 4Department of Biomedical Engineering, Cornell University
Synopsis
Differentiation MS lesions from ischemic demyelinating lesions is important because of their totally different treatment strategies. Our results suggested that the increased susceptibility of demyelinating lesions, the presence of QSM-ring lesions and the central vein in the lesions helped to differentiate MS lesions from ischemic demyelinating lesions. Thus, QSM provided the underling iron-related pathogenesis of MS lesions, which enable to differentiate MS lesions from ischemic demyelinating lesions.
Purpose
Ischemic demyelinating lesions become more and more common findings in the younger adults with increasing incidence of diabetes and hypertension in younger ages. Ischemic demyelinating lesions usually appear T2-hyperintense on MRI, which mimic the inflammatory demyelinating lesions, such as multiple scelerosis. However, it is essential for differentiating them in clinic because of the totally different treatment. Abnormal iron deposit was reported in MS lesions1, especially at the rim. Lots of MS lesions were found around vessels pathologically, resulting in a hypothesis that MS lesions originate from vessels. Both iron and deoxyhemoglobin in vessels are strong paramagnetic, resulting in increased susceptibility value on quantitative susceptibility mapping (QSM). QSM is a novel post-processing method for susceptibility weighted imaging, which is sensitive to magnetic phase change and enable qualitative and quantitative measurement of tissue susceptibility2. Therefore, we aim to differentiate the ischemic demyelinating lesions from MS lesions by qualifying and quantifying iron content using QSM.Methods
A total of 51 clinically confirmed MS patients and 20 ischemic patients, who underwent a MRI exam including a multi-echo gradient echo (GRE) sequence, were selected in this IRB approved retrospective study. QSM was reconstructed from GRE data. All images were co-registered to QSM. T2 hyper-intense lesions in MS patients were assumed to be MS lesions. T2 hyper-intense lesions in ischemic patients were assumed to be ischemic demyelinating lesions. White matter regions without an abnormal signal on all images were assumed to be normal white matter (NWM). For each T2 hyper-intense lesion, QSM was reviewed and labeled as hyper-intense, iso-intense and hypo-intense using local or mirror normal appearing white matter as reference. In addition, a T2 hyper-intense lesion was noted as QSM-ring lesion if there is a hyper-intense rim on QSM. A T2 hyper-intense lesion with central vein was also noted if a central vein can be identified across through the lesion on QSM. ROIs of MS lesions and ischemic demyelinating lesions were segmented on T2-weighted images. The ROIs were overlaid onto QSM and the susceptibility values of demyelinating lesions were calculated with the susceptibility of NWM as reference for each patient. The signal intensity of T2 lesions on QSM, the presence of QSM-ring lesion and the central vein were compared between MS patients and ischemic patients. The significance of difference in susceptibility value between MS lesions and ischemic demyelinating lesions was assessed by t-test.Results
A total of 376 MS lesions were identified in 51 MS patients, in which 272 lesions (72.34%) were hyper-intense on QSM and the other 104 lesions (27.66%) were iso-intense on QSM. Of the 376 MS lesions, 63 lesions (16.76%) were QSM-ring lesions, and 181 lesions (48.14%) were with central vein. A total of 326 lesions were identified in 20 ischemic patients, in which 43 lesions (13.19%) were slightly hyper-intense on QSM and the other 283 lesions (86.81%) were iso-intense on QSM. None of the ischemic demyelinating lesions were QSM-ring lesions, or with central vein. MS lesions showed more hyper-intense lesions on QSM than ischemic demyelinating lesions (p<0.05). The susceptibility value of MS lesions was significantly higher than that of ischemic demyelinating lesions (29.18 ± 19.94ppb vs. 11.2 ± 8.72ppb, p<0.001).Discussion and Conclusion
Our results suggested that the increased susceptibility of demyelinating lesions, the presence of QSM-ring lesions and/or the central vein in the lesions helped to differentiate MS lesions from ischemic demyelinating lesions. MS is an autoimmune inflammatory demyelinating disease. Abnormal iron deposit in MS lesions, which was confirmed to be closely associated with iron-rich microglia/macrophage pathologically, leads to remarkable increase of susceptibility3. Compared to MS lesions, ischemic demyelinating lesions showed much less infiltration of inflammatory cells, which hardly lead to susceptibility variation4. Thus, QSM provided the underling iron-related pathogenesis of MS lesions, which enable to differentiate MS lesions from ischemic demyelinating lesions.Acknowledgements
This study is supported by Chinese National Natural Science Foundation No. 81401390 and Hubei Province National Natural Science Foundation No. 2014CFB150.References
1. Chen W, Gauthier SA, Gupta A, et al. Quantitative susceptibility mapping of multiple sclerosis lesions at various ages. Radiology. 2014;271(1):183-92.
2. Chen W, Zhu W, Kovanlikaya I, et al. Intracranial calcifications and hemorrhages: characterization with quantitative susceptibility mapping. Radiology. 2014;270(2):496-505.
3. Bagnato F, Hametner S, Yao B, et al. Tracking iron in multiple sclerosis: a combined imaging and histopathological study at 7 Tesla. Brain. 2011;134(Pt 12):3602-15.
4. Murray ME, Vemuri P, Preboske GM, et al. A quantitative postmortem MRI design sensitive to white matter hyperintensity differences and their relationship with underlying pathology. J Neuropathol Exp Neurol. 2012;71(12):1113-22.
Figures
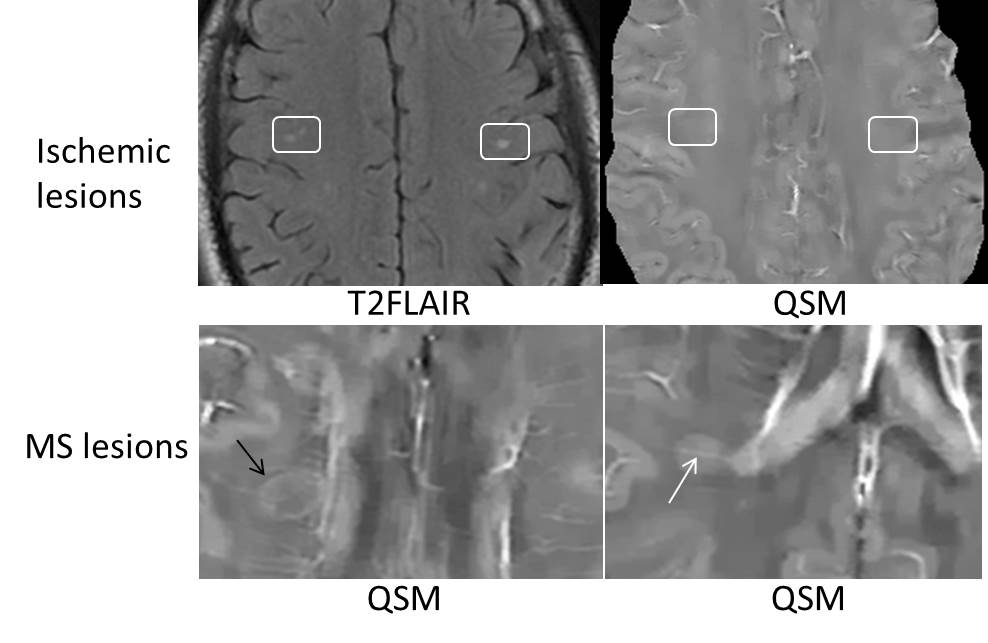
Fig.1. Ischemic demyelinating lesions showed hyperintense on T2FLAIR images and isointense on QSM (white boxes). While MS lesions showed obviously hyperintense on QSM, especially the presence of QSM-ring lesions (black arrow) and the central vein in the lesions (white arrow).
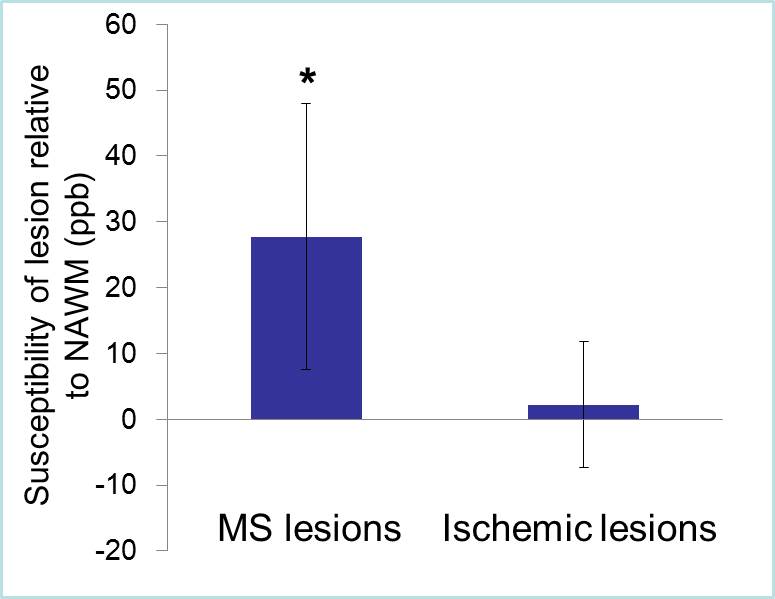
Fig.2. MS lesions showed higher susceptibility than ischemic demyelinating lesions (p<0.001).