2522
Evaluation of cervical carotid plaque volume using 3D T1 black-blood MRI : Comparison of manual measurement and automated measurement by the software.1Department of Radiology, Mie University Hospital, Mie, Japan, 2Department of Advanced Diagnostic Imaging, Mie University School of Medicine, Mie, Japan, 3Department of Electronic and Computer Engineering, Ritsumeikan University, Shiga, Japan, 4Department of Radiology, Mie University School of Medicine, Mie, Japan
Synopsis
Quantitative assessment of carotid plaque burden is required to monitor the effects of treatments for carotid atherosclerosis. Cervical carotid plaque volume in 13 patients with carotid artery stenosis was measured and evaluated using manual and automated software methods for 3D T1 black-blood MRI. Measurement reproducibility was better using the automated method than that using the manual method. The automated software developed for the measurement of carotid plaque volume was feasible and reliable and could significantly reduce the measurement time. This method appears to be of great value in clinical settings.
INTRODUCTION
Three dimensional T1 black-blood MRI (3D T1 BB MRI) is widely used in clinical settings. This method may be useful for measuring plaque volume in cases of carotid artery stenosis because the method’s improved anatomical coverage with retrospective visualization of the vessel wall using multiplanar reconstruction. Previously, investigators manually measured carotid-plaque volume to monitor the progression of atherosclerotic carotid plaque in patients receiving statin therapy [1] or to evaluate the carotid plaque burden in patients before carotid artery stenting [2]. However, manually measuring plaque volume is painful and time consuming. Therefore, we developed a software to automate the measurement of carotid-plaque volume.PURPOSE
The aim of this study was to compare manual and automated measurements of plaque volume in cervical carotid atherosclerosis and to assess the feasibility and the clinical usefulness of the automated software for the measurement of plaque volume in clinical settings.MATERIALS AND METHODS
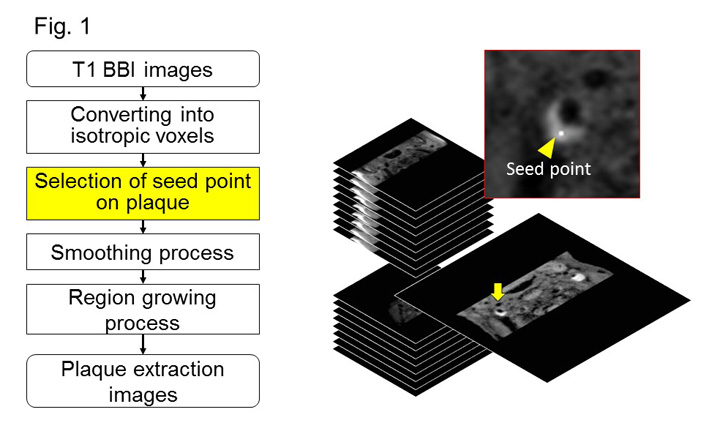
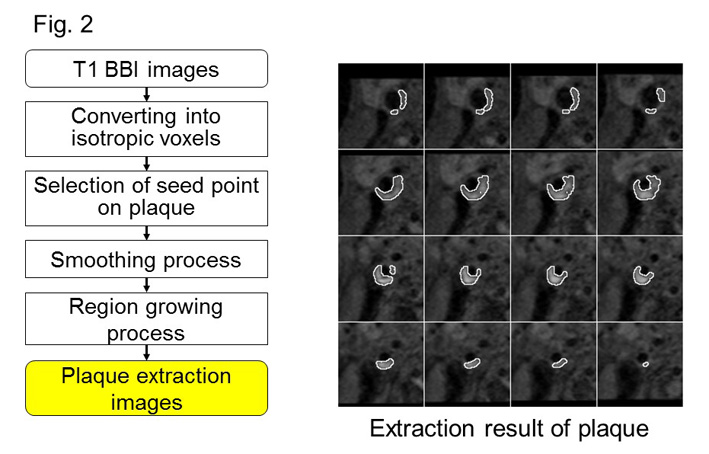
Thirteen patients with high-signal plaque in the cervical carotid arteries (mean age: 76 years) were studied to compare manual and automated measurements of carotid plaques. We used 3T MRI (Ingenia, Philips Healthcare, Best, Netherlands) with a dS HeadNeckSpine coil for imaging. The imaging-sequence parameters of 3D T1 BB MRI were: T1-VISTA, TR/TE = 350/23, refocusing angle = 40°, matrix = 0.45 × 0.45 × 0.90 mm, and scan time = 4 min 23 s. With the automation software, T1 BB images were converted into isotropic voxels. A seed point was manually selected in the center of a carotid plaque (Fig. 1). After the software performed smoothing and region-growing processes, plaque extraction images were obtained (Fig. 2). The plaque volume was calculated based on these images. Regarding data analyses, plaque volume was independently measured by two “raters” using the manual method and the software. Analyses of data obtained by the manual and automated methods for plaque-volume measurement included assessment of reproducibility regarding inter-raters and intra-raters and assessment of validity. Spearman’s rank correlation and Bland–Altman analysis were used for statistical analyses. In addition, measurement time was assessed for the manual and automated methods.RESULTS
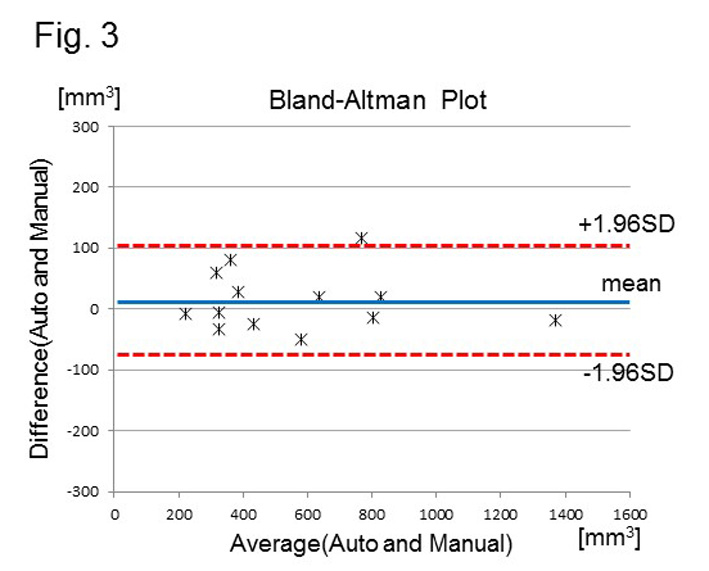
Reproducibility of the manual method showed intraclass correlation coefficients (ICC) of 0.986 in intra-raters and ICC of 0.98 in inter-raters. Reproducibility of the automated method showed ICC of 1.00 in intra-raters and ICC of 0.999 in inter-raters. A Bland–Altman analysis of the data showed that validity of the automated method was significant (r = 0.945, Fig. 3). Measurement time was much shorter with the automated method than that with the manual method (81.7 ± 7.8 vs. 189.5 ± 49.6 seconds, p < 0.01).DISCUSSION
We have shown that the developed automated software for the measurement of carotid-plaque volume is feasible and reliable in clinical settings. There was a significant correlation between the plaque volumes measured by the manual and the automated methods. Measurement reproducibility was better with the automated method. The automated software could significantly reduce the measurement time and it appears to be of great value in clinical settings.Acknowledgements
No acknowledgement found.References
1. Boussel L, et al. Atherosclerotic plaque progression in carotid arteries: monitoring with high-spatial-resolution MR imaging--multicenter trial. Radiology 2009, 252: 789-96.
2. Tanemura H, et al. High-risk plaque for carotid artery stenting evaluated with 3-dimensional T1-weighted gradient echo sequence. Stroke 2013, 44: 105-10.
Figures