2476
Decreased axial diffusivity in early Parkinson’s disease subjects: Insights from Parkinson’s Progressive Markers Initiative (PPMI) dataset1Cleveland Clinic Lou Ruvo Center for Brain Health, Las Vegas, NV, United States
Synopsis
In vivo imaging that reliably captures the impact of the spreading pathology of Parkinson’s disease (PD), including its impact on both white and gray matter, remains elusive. In this study, we performed skeleton-wise analysis of multi-site DTI data from a cohort of early PD-subjects in Parkinson’s Progressive Markers Initiative (PPMI) database. Tract-based-spatial-statistics analysis revealed three clusters mainly located in corticospinal tract, and superior frontal gyrus that had a lower AxD in early PD-subjects suggesting DTI measures can be used to differentiate controls and early
Introduction
The pathologic development of Parkinson’s disease (PD) appears to be related to the spread of abnormal synuclein in a largely caudal-rostral direction in the CNS1–3. In vivo imaging that captures the impact of this spreading pathology on both white and gray matter remains elusive4,5. Diffusion tensor imaging (DTI) is capable of delineating in vivo microstructural changes of white matter tracts noninvasively. DTI can detect alterations in white matter in early stages of PD4, with potential to develop into important biomarker in understanding PD. However, studies utilizing either voxelwise comparisons or skeleton-wise comparisons have produced conflicting conclusions in diffusion derived measures of the same region4. Moreover, most of the studies with early PD suffer from low sample size resulting in low statistical power which may also contribute to conflicting results. In this study, we performed skeleton-wise analysis of multi-site DTI data from a cohort of early PD-subjects in Parkinson’s Progressive Markers Initiative (PPMI) database6 and showed lower axial diffusivity (AxD) in PD as compared to controls.Methods
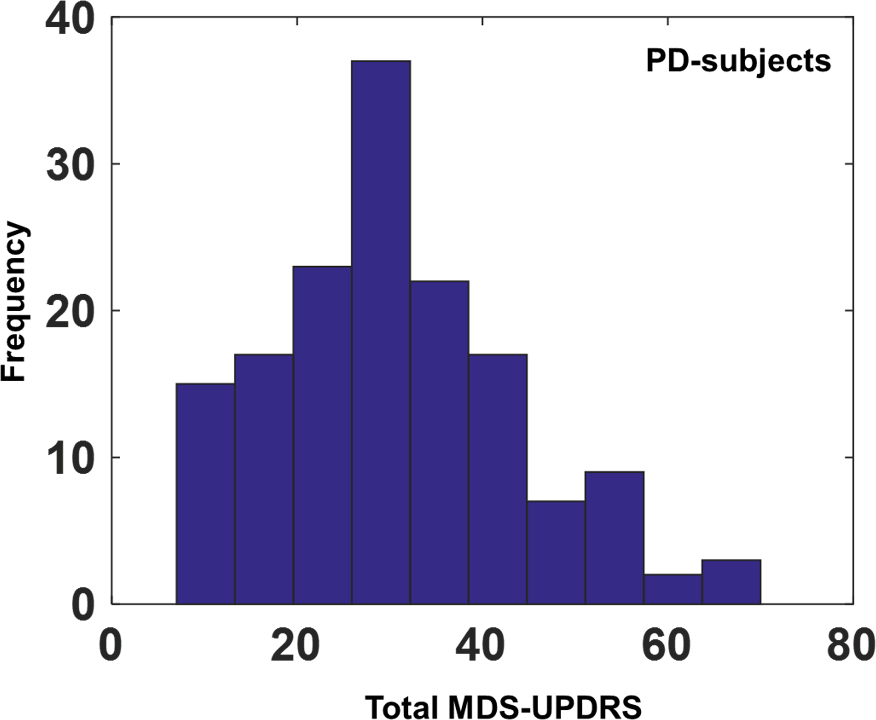
Subjects: Diffusion-MRI data from PPMI database from 70 (24 female) healthy controls (age: 60.37±10.72years, years of education (YOE): 15.64±3.06years) and 152 early PD-subjects (54 female) (age: 61.01±9.2years, (YOE): 15.15±2.94years, total MDS-UPDRS: 30.75±12.99, disease duration: 7±7.11months) was used in this study. Imaging parameters are described in detail at http://www.ppmi-info.org/6. Only data from 3T Siemens scanners with the first visit were used to ensure uniformity of diffusion data. Voxelwise analysis: Tract-based spatial statistics (TBSS)7 from FSL was used for voxelwise comparisons between controls and PD for various diffusion derived metrics such as fractional anisotropy (FA), AxD, radial diffusivity (RD), and mean diffusivity (MD). Voxelwise analysis was also conducted to investigate association of disease progression and duration with various diffusivity measures in PD-subjects. Statistical analysis: Nonparametric permutation testing with various confounds such as age, gender, years of education, and total brain volume was conducted using randomise8 in FSL. The significant voxels were clustered using the cluster command in FSL9 and various diffusion derived metrics were extracted for each cluster. Linear regression analysis was conducted between the diffusion derived metrics in each cluster and disease duration and severity (as measured by UPDRS score) after controlling for confounds.Results
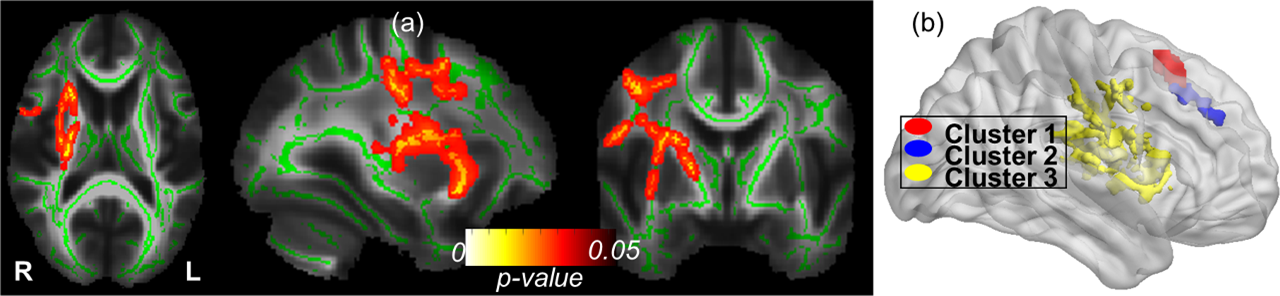
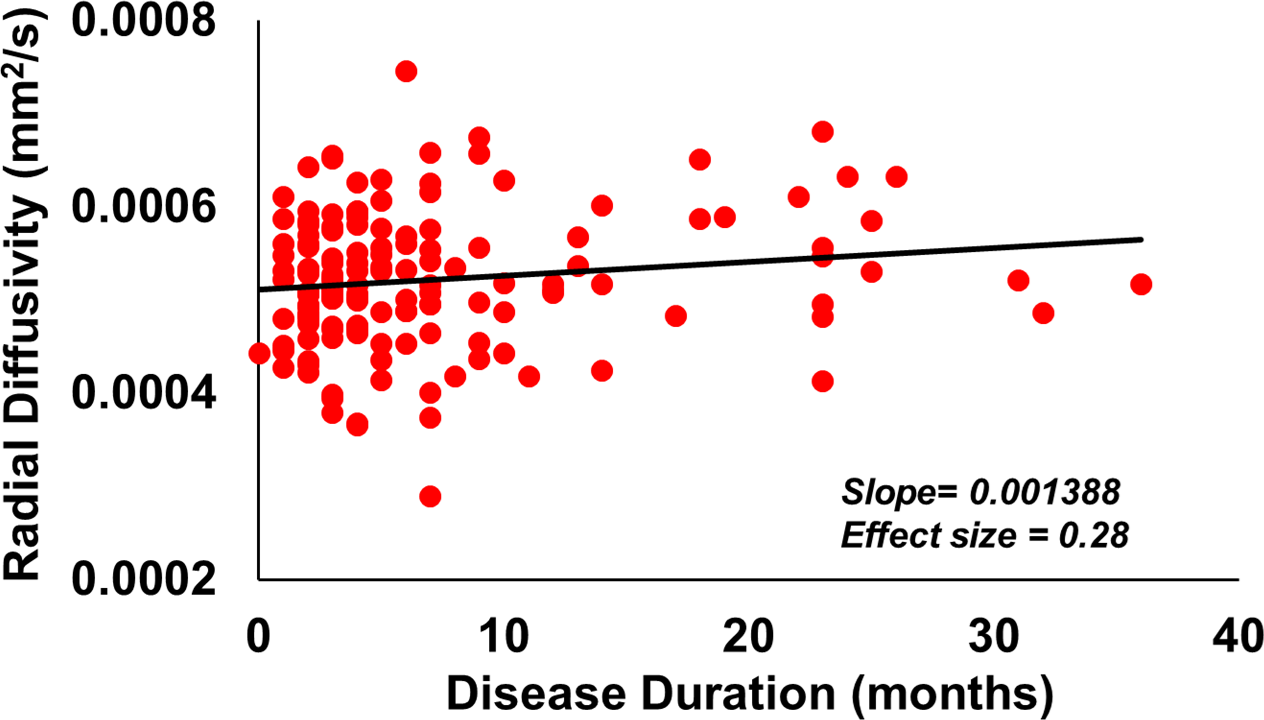
Fig.1 shows the distribution of total MDS-UPDRS. Regions with significantly greater AxD in controls are overlaid on the white matter skeleton derived from mean FA of all the subjects used in this study (Fig.2 (a)). White matter tracts with significantly reduced AxD in PD comprises mainly of the corticospinal tracts, superior longitudinal fasciculus, and internal and external capsule. There were three clusters with peak statistic located in paracingulate cortex (38 voxels), superior frontal gyrus (139 voxels), and external capsule (2887 voxels) as shown in Fig.2 (b). None of the other diffusivity measures showed any significant differences between controls and PD, but RD showed a significant positive association with disease duration (slope=0.0014, effect size=0.28) in the voxels comprising cluster 1 (Fig.3).Discussion
Using multi-site DTI data from a cohort of early PD-subjects, we found that only AxD can be reliably detected to have any significant difference from controls. Our results further show that only RD showed positive association with disease duration but no other diffusivity measures showed any association with disease severity. Increased RD is usually associated with demyelination10 and has been shown to correlate with clinical scores of PD-subjects11. Voxelwise statistical comparisons with either disease severity or disease duration revealed no association with any diffusivity measures, suggesting that disease variability may have an important role and may be smoothing of the data should be performed before statistical analysis to improve the sensitivity of TBSS analysis12. Future studies will evaluate the role of tensor based registration13 instead of FA based registration as used by TBSS, and performing both voxelwise and skeleton-wise analysis in the same dataset to investigate the role of registration algorithms, and smoothing effects14 on detecting differences in diffusivity measures between controls and early PD-subjects.Conclusion
TBSS analysis revealed three clusters mainly located in corticospinal tract, superior frontal gyrus, and paracingulate cortex that had a lower AxD in early PD-subjects. Moreover, RD in the cluster showed a significantly positive association with disease duration suggesting DTI measures can be used to differentiate controls and early PD and can be further exploited to understand its role in disease progression and severity.Acknowledgements
The study was supported in parts by National Institute of General Medical Sciences (grant: P20GM109025) and the Elaine.P.Wynn and family foundation.References
1. Braak H, Del Tredici K, Rub U, de Vos RAI, Jansen Steur ENH, Braak E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging 2003; 24: 197–211.
2. Braak H, Bohl JR, Muller CM, Rub U, de Vos RAI, Del Tredici K. Stanley Fahn Lecture 2005: The staging procedure for the inclusion body pathology associated with sporadic Parkinson’s disease reconsidered. Mov Disord 2006; 21: 2042–51.
3 . Goedert M, Spillantini MG, Del Tredici K, Braak H. 100 years of Lewy pathology. Nat Rev Neurol 2013; 9: 13–24.
4. Hall JM, Ehgoetz Martens KA, Walton CC, et al. Diffusion alterations associated with Parkinson’s disease symptomatology: A review of the literature. Parkinsonism Relat Disord 2016; published online Sept. DOI:10.1016/j.parkreldis.2016.09.026.
5. Pyatigorskaya N, Gallea C, Garcia-Lorenzo D, Vidailhet M, Lehericy S. A review of the use of magnetic resonance imaging in Parkinson’s disease. Ther Adv Neurol Disord 2014; 7: 206–20.
6. www.ppmi-info.org.
7. Smith SM, Jenkinson M, Johansen-Berg H, et al. Tract-based spatial statistics: Voxelwise analysis of multi-subject diffusion data. Neuroimage 2006; 31: 1487–505.
8. Smith SM, Nichols TE. Threshold-free cluster enhancement: Addressing problems of smoothing, threshold dependence and localisation in cluster inference. Neuroimage 2009; 44: 83–98.
9. Jenkinson M, Beckmann CF, Behrens TEJ, Woolrich MW, Smith SM. FSL. Neuroimage 2012; 62: 782–90.
10. Alexander AL, Lee JE, Lazar M, Field AS. Diffusion Tensor Imaging of the Brain. Neurotherapeutics 2007; 4: 316–29.
11. Auning E, Kjaervik VK, Selnes P, et al. White matter integrity and cognition in Parkinson’s disease: a cross-sectional study. BMJ Open 2014; 4: e003976.
12. Rae CL, Correia MM, Altena E, Hughes LE, Barker RA, Rowe JB. White matter pathology in Parkinson’s disease: The effect of imaging protocol differences and relevance to executive function. Neuroimage. 2012; 62: 1675–84.
13. Zhang H, Yushkevich PA, Alexander DC, Gee JC. Deformable registration of diffusion tensor MR images with explicit orientation optimization. Med Image Anal 2006; 10: 764–85.
14. Jones DK, Symms MR, Cercignani M, Howard RJ. The effect of filter size on VBM analyses of DT-MRI data. Neuroimage 2005; 26: 546–54.
Figures