2463
Intracranial plaque imaging using reduced field of view 3D fast spin echo1GE healthcare MR Research China, Beijing, People's Republic of China, 2Wuhan Children Hospital, 3PLA Army General Hospital
Synopsis
In this study, the use use of reduced FOV CUBE is studied in comparison to full FOV CUBE as well as other common techniques. It was seen that CUBE sequences provide robust and superior image details and black blood effects, due to the advantageous 3D FSE acquisition. With only 1/4 of the FOV acquired, reduced FOV CUBE may complete the scan using half of the scan time (using twice Nex) while obtaining highly consistent results as FF CUBE. Reduced FOV CUBE may also reduce the motion related artifacts that may affect the homogeneity of the lumen area.
Purpose
Intracranial plaque is a leading cause of hemorrhage, the screening and diagnosis of plaque need both morphological and compositional assessment. The former requires the use of high resolution black blood acquisition to differentiate between plaque, vessel wall and lumen, the latter requires multi-contrast acquisitions for differentiation among hemorrhage, lipid core, calcification and fiber[1]. 3D FSE based acquisition, such as SPACE and CUBE, has been shown to be suitable for plaque imaging due to their high SNR, low distortion and black blood effects. Furthermore, it is capable of T1, T2 and T1 enhanced acquisitions that facilitate image registrations. However, conventional 3D FSE acquisition is challenged by the relatively long acquisition time, which not only reduces the patient comfort level and also increases the motion vulnerability. Since plaque imaging is in general only concerned with the bifurcation of the arteries, the actual volume of interest is rather limited. In this work, we investigate the use of reduced field of view (rFOV) 3D FSE acquisition [2] for intracranial plaque imaging.Method
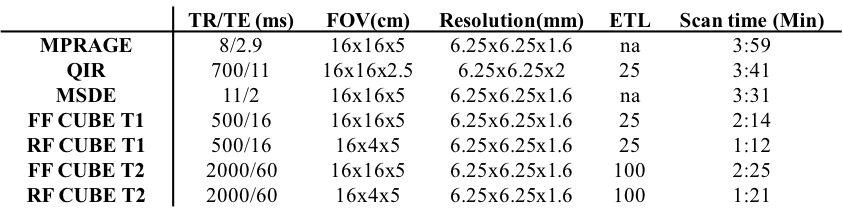
4 patients pre-diagnosed with plaque using ultrasound or CT angiography participated in this study, consent forms were obtained. All the participants underwent the following scans on a 3.0T scanner (MR 750, GE) using an 8-channel dedicated plaque coil: MSDE, QIR FSE, MPRAGE, full FOV (FF) CUBE T1, reduced FOV (RF) CUBE T1, FF CUBE T2, RRF CUBE T2 (Table 1). Image analysis was focused on two aspects: the contrast to noise ratio (CNR) and dimensions of the plaque. The CNRs were calculated as (plaque-lumen)/lumen for all the sequences; the dimensions of the plaque were measured slice-wise and compared between CUBE and rFOV CUBE. Lumen and plaque regions were identified semi-automatically using a signal intensity based regional growth approach by an experienced radiologist. The ROIs were identified on CUBE and copied to different contrasts, given identical FOV and in plane resolutions were used.Results
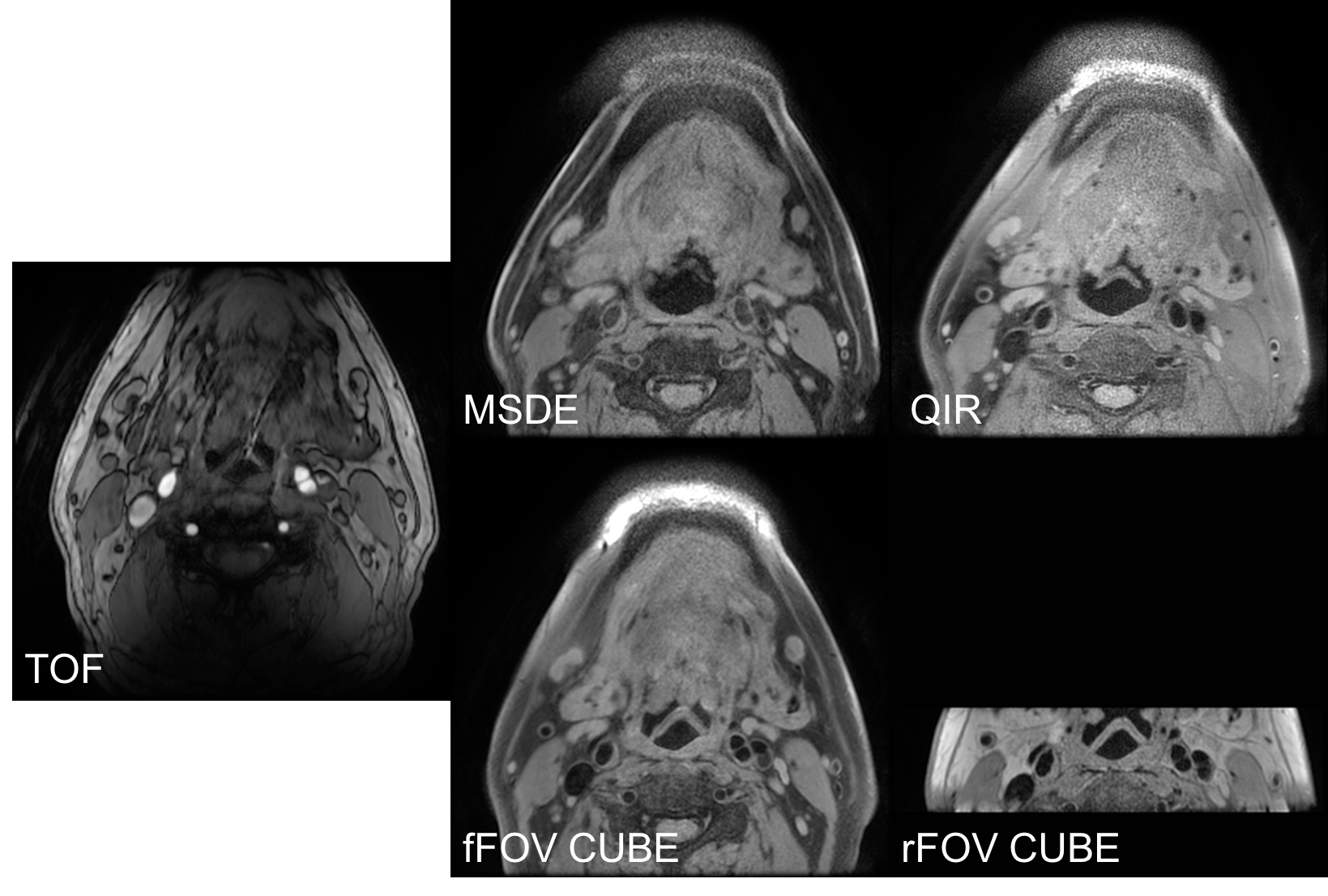
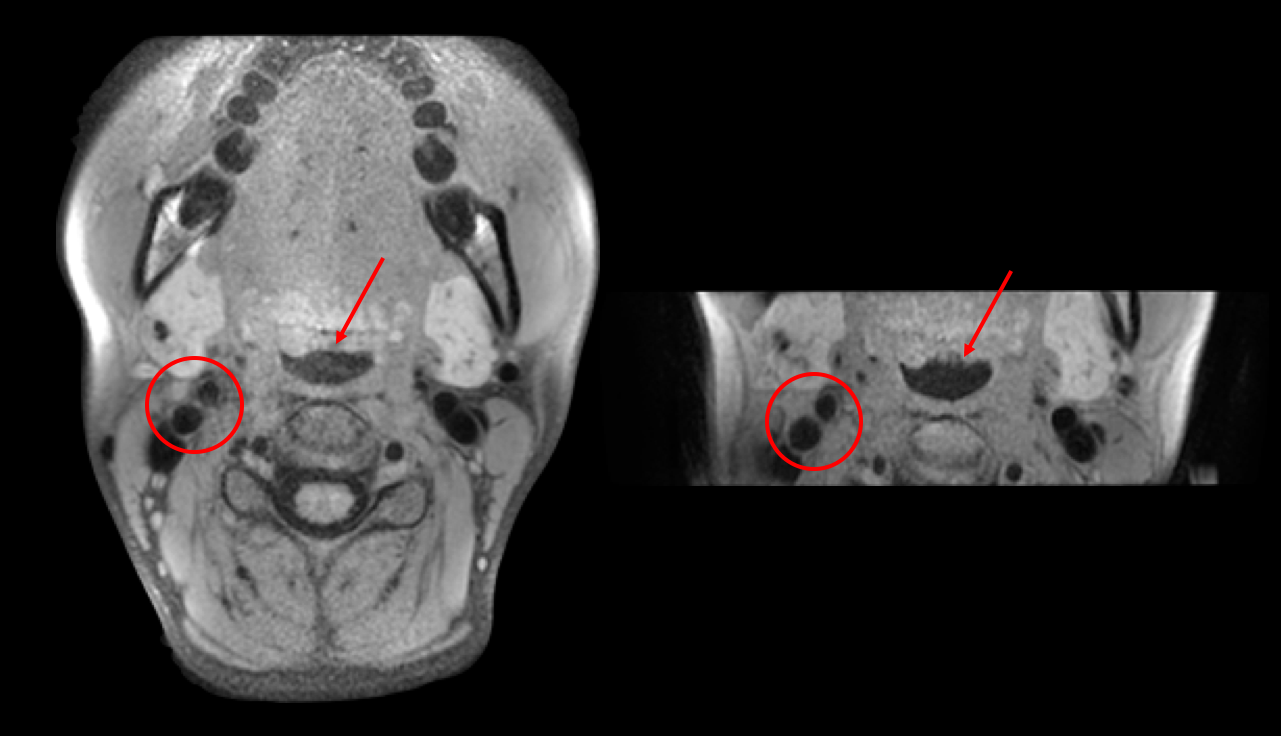
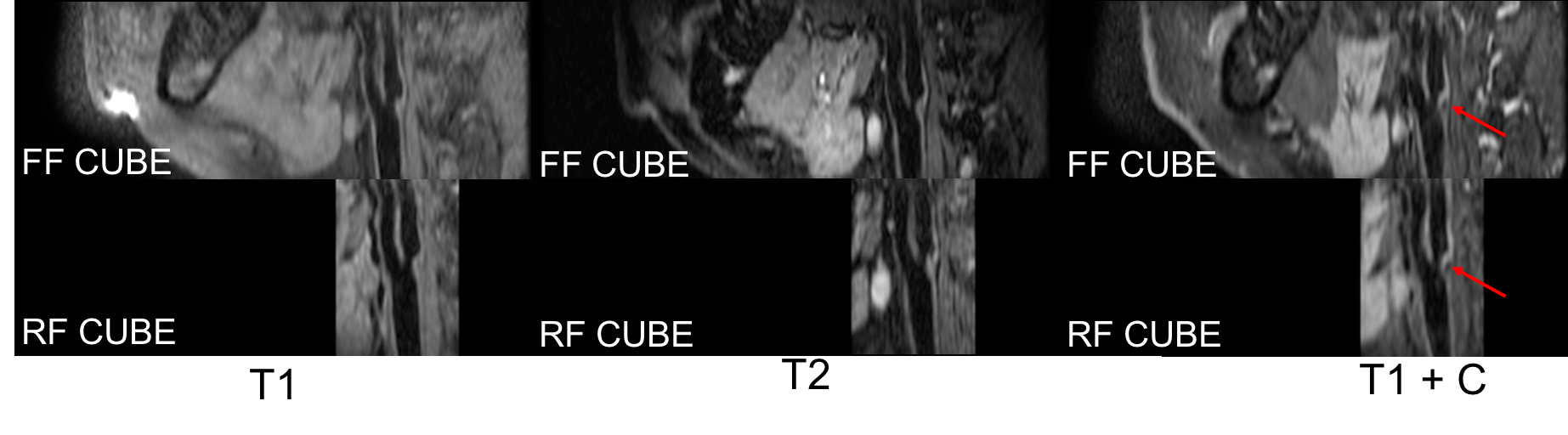
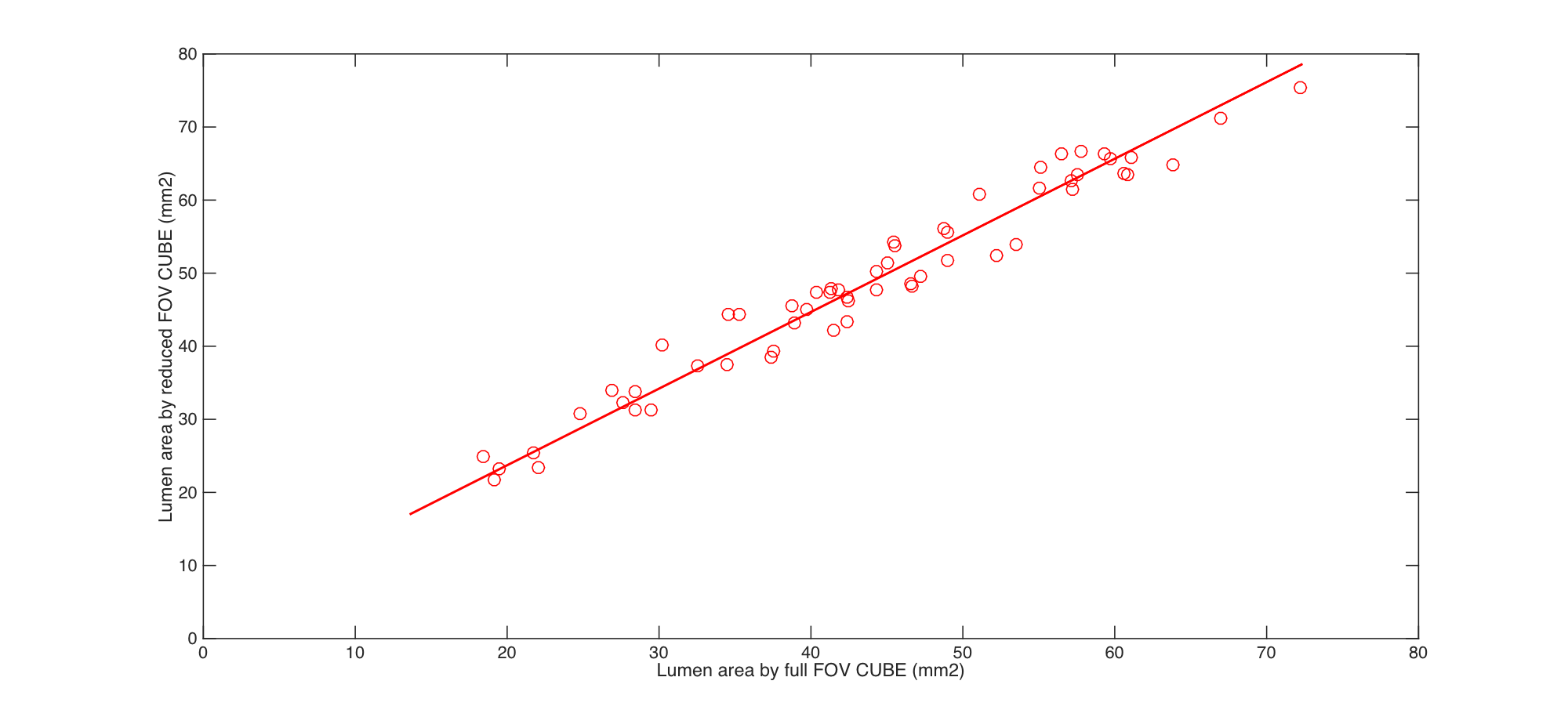
An axial slice with the presence of plaque in the same patient from different sequences are shown in Fig.1. It is seen that CUBE acquisitions provided relatively higher level of SNR; CUBE acquisitions also led to superior suppression of the blood as seen by dark lumen areas. The measured CNRs for MSDE, QIR, MPRAGE, FF CUBE T1 and RF CUBE T1 were 21.3, 23.5, 22.7, 33.4, 36.2 respectively. The sagittal slice images of the same patient of full FOV and reduced FOV CUBE T1, T2, T1 contrast are shown in Fig.2. It can be seen that morphological dimensions as well as different compositions were well depicted, the hypo-intense region in contrast enhanced T1 indicated the presence of calcification. Fig.3 illustrates a case where motion induced artifacts were present in the lumen (circled), which may be mistaken as plaque. The arrowed region also suggested much stronger motion artifacts in the FF CUBE. The scatter plot of the measured lumen areas in different axial slices obtained using full FOV and reduced FOV acquisitions is shown in Fig.4, a high correlation coefficient of 0.94 was obtained.Discussion and conclusion
Intracranial plaque imaging conveys great clinical significance, and many techniques have been developed for its needs. In this study, the use use of reduced FOV CUBE is studied in comparison to full FOV CUBE as well as other common techniques. It was seen that CUBE sequences provide robust and superior image details and black blood effects, due to the advantageous 3D FSE acquisition. With only 1/4 of the FOV acquired, RF CUBE may complete the scan using half of the scan time (using twice Nex) while obtaining highly consistent results as FF CUBE. In this study, even higher lumen CNR was obtained using RF CUBE, as the lumen areas in FF CUBE may be contaminated by motion artifacts in FF CUBE. The decreased scan time may be used improving patient comfort and reducing vulnerability to motion as demonstrated, or higher spatial resolution may be obtained improving the depiction of the vascular structures. The multi-contrast compatibility of RF CUBE and its short scan time (that facilitates image registration) would be of great clinical value of intracranial plaque imaging.Acknowledgements
No acknowledgement found.References
[1] J. Wang, et al., Simultaneous Noncontrast Angiography and intraPlaque hemorrhage (SNAP) Imaging for Carotid Atherosclerotic Disease Evaluation, MRM, 2013:69.
[2] M. Han, et al., Variable flip angle three-dimensional fast spin-echo sequence combined with outer volume suppression for imaging trabecular bone structure of the proximal femur. JMRI, 2015:41(5).
Figures