2455
Association of Atherosclerotic Plaque Characteristics between Intracranial and Extracranial Carotid Arteries in Symptomatic Patients: A 3D Multicontrast MR Vessel Wall Imaging Study1Department of Radiology, Beijing Tsinghua Changgung Hospital, Tsinghua University, Beijing, People's Republic of China, 2Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University, Beijing, People's Republic of China, 3Department of Radiology, University of Washington, Seattle, United States, 4Philips Research China, Philips Healthcare, Beijing, People's Republic of China, 5Department of Radiology, PLA General Hospital, Beijing, People's Republic of China
Synopsis
This study investigated the correlation between intracranial and extracranial carotid artery atherosclerotic disease in symptomatic patients. We found that extracranial artery disease showed larger plaque burden than intracranial artery disease. In addition, the number of extracranial plaques was found to be associated with intracranial plaque number and maximum wall thickness (MaxWT) and the extracranial carotid MaxWT was independently associated with intracraninal artery stenosis. The association of extracranial artery plaque number and MaxWT with severity of intracranial artery disease suggests that the plaque burden measurements in extracranial carotid arteries might be effective indicators for the severity of intracranial atherosclerosis.
Introduction and Purpose
It has been shown that intracranial atherosclerotic disease (ICAD) is the major cause of ischemic stroke in Chinese population [1]. Clinically, angiography is the major approach for diagnosis of ICAD but this technique will underestimate plaque severity due to lacking of vessel wall information. Recently, high resolution MR imaging (HRMRI) has been largely utilized to characterize ICAD. However, using HRMRI to evaluate ICAD is challenging due to the limited spatial resolution and insufficient suppression of cerebral spinal fluid. As a systemic disease, atherosclerosis commonly involves multiple vascular beds simultaneously and the co-existing atherosclerosis in intracranial and extracranial carotid arteries has been found to be prevalent in stroke patients [2]. Most recently, 3D multicontrast MR vessel wall imaging techniques have been proposed [3] which have the potential to comprehensively characterize intracranial and extracranial carotid artery atherosclerosis simultaneously. We hypothesized that extracranial carotid artery atherosclerosis might be a surrogate for assessing the ICAD. This study sought to investigate the relationship of atherosclerotic disease between intracranial and extracrnaial carotid arteries using HRMRI.Methods
Study sample: Patients with recent cerebrovascular symptoms and carotid plaque determined by ultrasound were recruited. MR imaging: All patients underwent cerebrovascular wall MR imaging on a 3.0T MR scanner (Phillips, Achieva TX) with custom-designed 36-channel neurovascular coil. A 3D multicontrast vessel wall imaging protocol was conducted to acquire MERGE, SNAP and T2-VISTA sequences with the following parameters: 3D MERGE: fast field echo (FFE), TR/TE 9.2/4.3ms, flip angle 6°; 3D SNAP: FFE, TR/TE 9.9/4.8 ms, flip angle 11/5°; and 3D T2-VISTA: turbo spin echo (TSE), TR/TE 2500/278 ms, flip angle 90°. All 3D imaging sequences were acquired coronally with the same field of view of 40×160×250mm3 and isotropic spatial resolution of 0.8×0.8×0.8mm3. Image review: Two experienced radiologists reviewed the MR images with consensus. Presence/absence of atherosclerotic plaque in intracranial or extracranial carotid artery was determined. The maximum wall thickness (MaxWT), length, and stenosis of each plaque were measured. The presence/absence of calcification, lipid-rich necrotic core (LRNC), and intraplaque hemorrhage (IPH) for each plaque was assessed. Statistical analysis: The characteristics of plaques between intracranial and extracranial carotid arteries were compared and their correlations were analyzed.Results
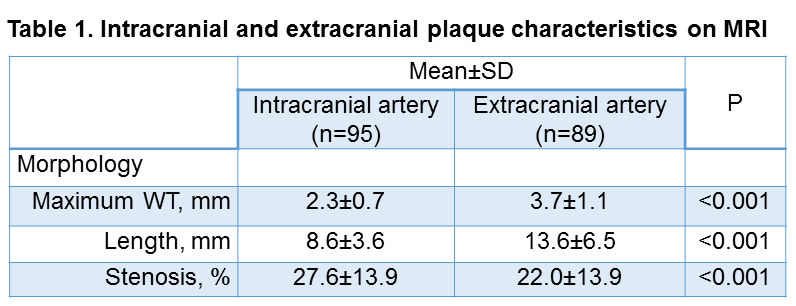
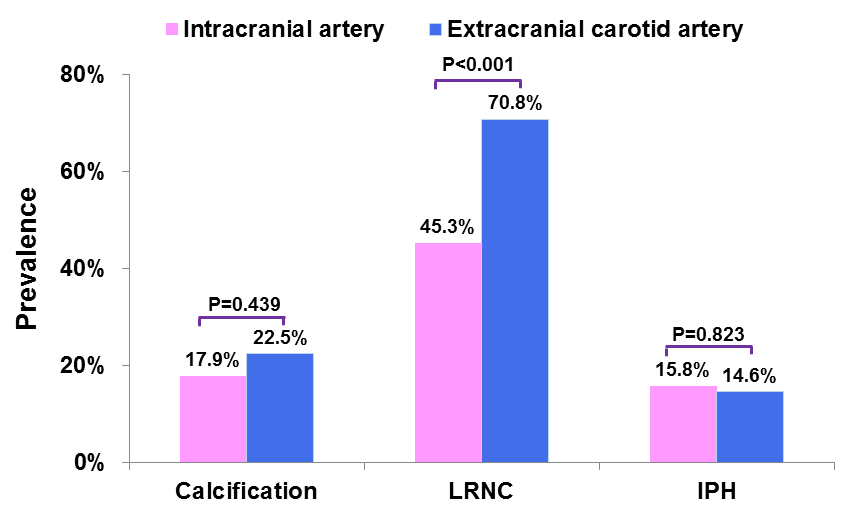
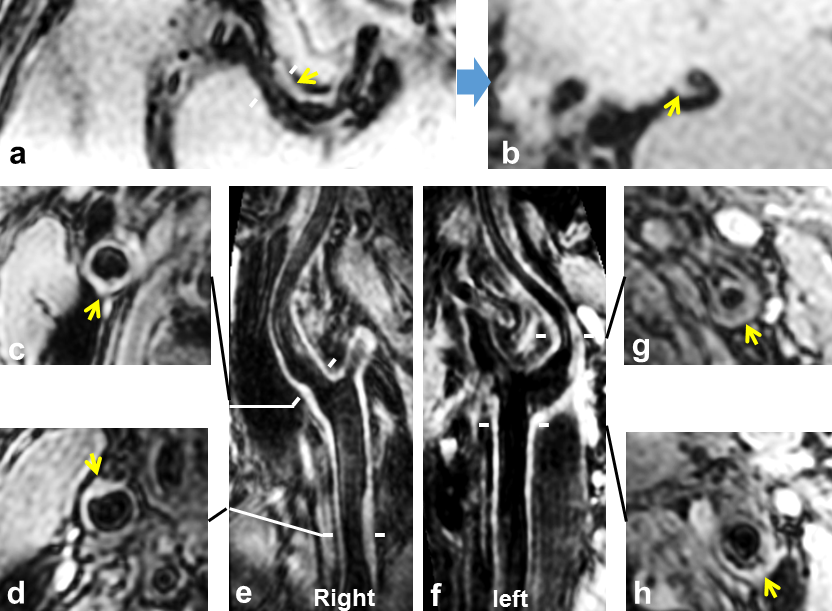
In total, 45 patients (mean age: 58.3±8.5 years, 30 males) were recruited and 184 atherosclerotic plaques were detected (intracranial plaque=95, and extracranial plaque=89). The MaxWT, length, and stenosis of extracranial carotid plaques were significantly larger than those of intracranial plaques (all p<0.001, Table 1). Compared with intracranial plaques, extracranial carotid artery plaques showed significantly greater prevalence of LRNC (70.8% vs. 45.3%, p<0.001) but this difference was not found in prevalence of calcification and IPH (all p>0.05) (Figure 1). Significant correlations were found in presence of calcification (r=0.355, p=0.017) and plaque number (r=0.311, p=0.037) between intracranial and extracranial carotid arteries. The plaque number of extracranial carotid artery was significantly associated with the MaxWT of intracranial plaques (r=0.307, p=0.040). Figure 2 represents an example showing multiple plaques in extracranial carotid arteries and an atherosclerotic plaque in right middle cerebral artery in the same patient. In predicting intracranial severe stenosis (>50% stenosis), the odds ratio (OR) of MaxWT in extracranial carotid arteries with increment of 1 standard deviation was 2.278 (95% CI, 1.003-5.174, p=0.049) and 12.432 (95% CI, 1.175-131.481, p=0.036) before and after adjusted for confounding factors, respetively.Disccusion
This study investigated the correlation between intracranial and extracranial artery atherosclerotic disease in symptomatic patients. We found that extracranial carotid artery atherosclerotic disease showed larger plaque burden than intracranial artery disease. The prevalence of LRNC in extracranial carotid arteries was higher than that of intracranial arteries. In addition, we found the number of extracranial artery plaques was associated with intracranial artery plaque number and MaxWT. The plaque number may represent the atherosclerotic plaque burden. Similar results were also seen in patients with coronary artery disease. Investigators found the relationship between coronary plaque number and coronary events [4,5]. In addition, we found that the MaxWT of extracranial carotid artery plaques was independently associated with intracraninal severe stenotic disease. Our findings suggest that the plaque burden measurements in extracranial carotid artery might be effective indicators for the severity of intracranial atherosclerosis.Conclusion
The plaque burden measurements, particularly the plaque number and maximum wall thickness, in extracranial carotid artery might be effective indicators for the severity of intracranial atherosclerosis.Acknowledgements
None.References
[1] Wang Y, Zhao X, Liu L, et al. Prevalence and outcomes of symptomatic intracranial large artery stenoses and occlusions in China: the Chinese Intracranial Atherosclerosis (CICAS) Study. Stroke. 2014;45:663-669.
[2] Liu HM, Tu YK, Yip PK, et al. Evaluation of intracranial and extracranial carotid steno-occlusive diseases in Taiwan Chinese patients with MR angiography: preliminary experience. Stroke. 1996;27:650-653.
[3] Zhou Z, Li R, Zhao X, et al. Evaluation of 3D multi-contrast joint intra- and extracranial vessel wall cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2015;17:41.
[4] Stolzmann P, Donati OF, Desbiolles L, et al. Coronary artery plaques and myocardial ischaemia. Eur Radiol. 2011;21:1628-1634.
[5] Sato A, Ohigashi H, Nozato T, et al. Coronary artery spatial distribution, morphology, and composition of nonculprit vulnerable plaques by 64-slice computed tomography angiography in patients with acute myocardial infarction. Am J Cardilo. 2010;105:930-935.
Figures