2451
Triple Magnetic Resonance Angiography (triple-MRA) for confirmation of obliteration following Gamma Knife Radiosurgery for Arterial-Venous Malformations of the brain1The Gamma Knife Centre at Queen Square, National Hospital for Neurology and Neurosurgery, London, United Kingdom, 2Department of Neurosurgery, National Hospital for Neurology and Neurosurgery, London, United Kingdom, 3Neuroradiology Unit, Department of Diagnostic and Pathology, University Hospital of Verona, Verona, Italy, 4The Lysholm Department of Neuroradiology, National Hospital for Neurology and Neurosurgery, London, United Kingdom, 5Medical Physics and Bioengineering, University College London Hospital, London, United Kingdom, 6Academic Neuroradiological Unit, Department of Brain Repair and Rehabilitation, Institute of Neurology, University College London, London, United Kingdom, 7C. J. Gorter Center for High Field MRI, Department of Radiology, Leiden University Medical Center, Leiden, Netherlands, 8Radiology Unit, Department of Diagnostic and Pathology, University Hospital of Verona, Verona, Italy, 9Centre for Medical Imaging, University College London, London, United Kingdom, 10Department of Neuroscience, University Hospital of Verona, Verona, Italy
Synopsis
This study assesses whether a combination of three Magnetic Resonance Angiography (MRA) techniques, referred to as triple-MRA, can be used as an alternative to DSA for confirmation of AVM obliteration following GKR and to characterise residual AVMs in case of incomplete response.
The follow up DSA and triple-MRA of twenty-four patients were independently reviewed by two observers regarding the presence/absence of a residual AVM. Triple-MRA consistently agreed with DSA regarding the absence or presence of residual AVMs and proved to be highly suitable for characterisation of residual AVMs.
Objective
Arterio-Venous Malformations (AVMs) are congenital vascular abnormalities characterized by anomalous connections between arteries and veins leading to arteriovenous shunting through a network of coiled and tortuous vessels. Gamma Knife Radiosurgery (GKR) is a well-established minimally invasive treatment for brain AVMs. It produces gradual decrease in blood flow through the AVMs and after two to three years approximately 75% of them are completely obliterated.1
Intra-arterial Digital Subtraction Angiography (DSA) is still the reference standard for confirmation of obliteration following GKR of brain AVMs due to suboptimal sensitivity of standard MR angiography.2 However, DSA is invasive, it carries a potential risk of peri-procedural complications and exposes both patients and staff to ionizing radiation.3
This study aims to evaluate whether a combination of three Magnetic Resonance Angiography (MRA) techniques, referred to as triple MRA (triple-MRA), can be used as an alternative to DSA to confirm AVM obliteration following GKR and to characterise residual AVMs in case of incomplete response.
Methods
Twenty-four adult patients undergoing DSA for confirmation of obliteration following GKR for brain AVMs were included. They also underwent triple-MRA including 4D Arterial Spin Labelling based angiography (4D-ASL-MRA), High Definition Time-Of-Flight angiography (HD-TOF) and Contrast-Enhanced Time-Resolved MRA (CE-TR-MRA).
The mean AVM volume at the time of GKR was 7.76 ml (0.07-50.54). Eight AVMs were located in the temporal lobe, six were frontal, four parietal and two occipital. Four were deep seated (basal ganglia or midbrain). The mean time post-GKR was 50.5 months (27-168).
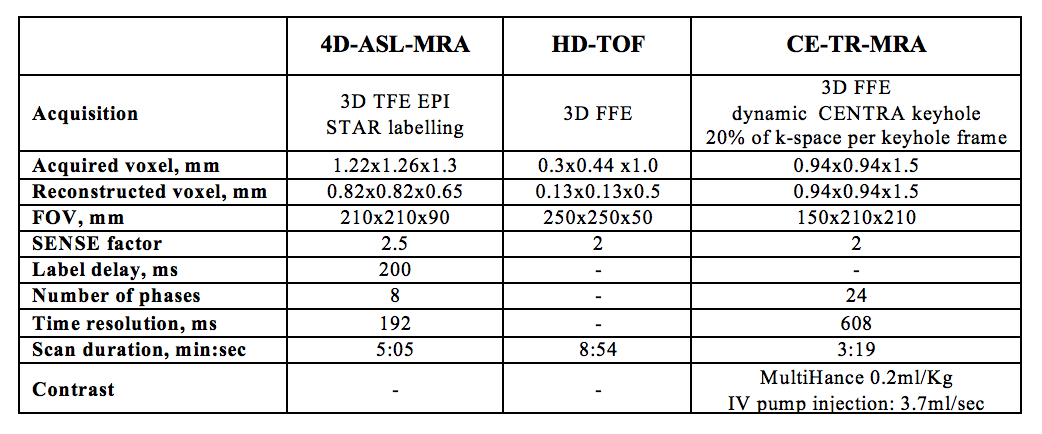
Triple-MRA was performed using a 3.0 T MRI system (Philips Healthcare Systems, Best, The Netherlands) with the parameters shown in table 1. Total triple-MRA scanning time 18:11mins. The DSA and triple-MRA were separately and blindly evaluated by two independent interventional neuro-radiologists (FBP and TS) regarding the presence/absence of a residual AVM. The Spetzler-Martin grading system (size: <3 cm, 3-6 cm and > 6 cm; venous drainage: deep vs superficial only; eloquence: eloquent vs. non-eloquent adjacent brain) was used to grade residual lesions on both imaging modalities and further characterisation of residual lesions included the identification of the feeding arteries and draining veins.
Results
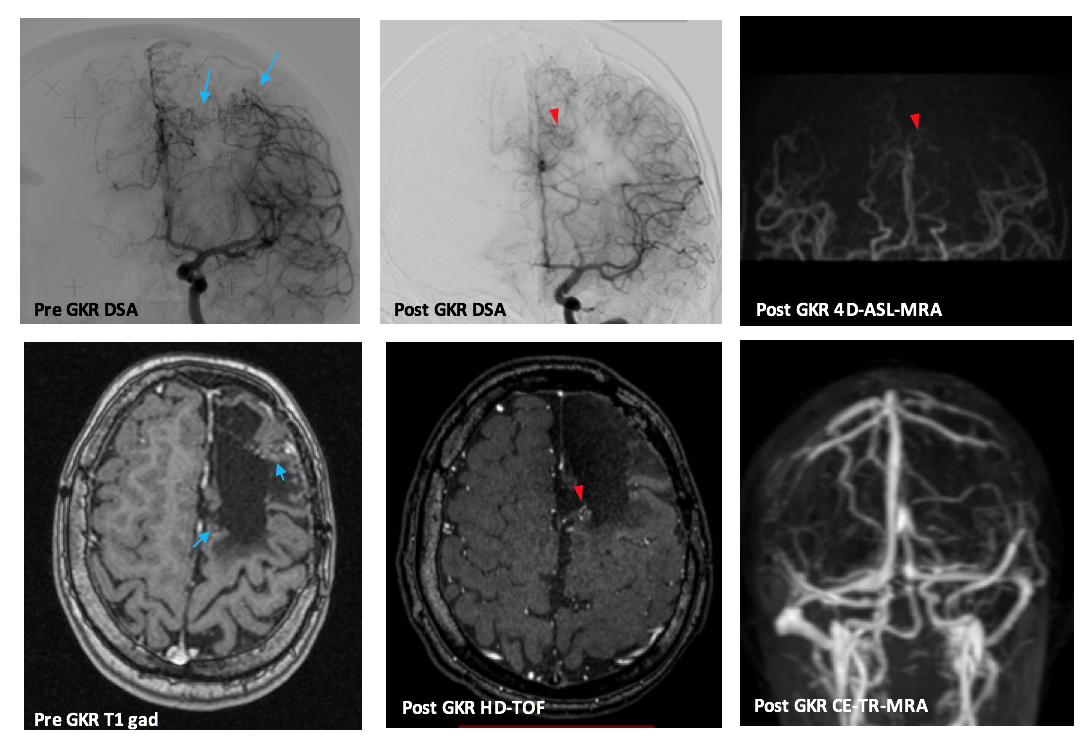
Triple-MRA demonstrated complete AVM obliteration in 16 patients and a residual AVM was noted in 8 subjects. This was in complete agreement with the DSA results by both observers and DSA clinical reports. Six of eight residual AVMs were clearly identified on all three MRA techniques. In two cases the residual lesion was noted on 4D-ASL-MRA and HD-TOF but not on CE-TR-MRA due to very small size of the residual lesion in one and the diffuse nature of the AVM nidus in the second case (Figure 1).
There was complete agreement on size and drainage scores of the Spetzler-Martin grading system for all residual AVMs between triple-MRA and DSA for the two observers. Different eloquence scores were given for two cases by the first observer and for three cases by the second observer. In the residual AVMs, observer 1 identified a total of thirteen feeding arteries both on DSA and triple-MRA, whereas observer 2 identified 17 feeding arteries on the DSA and 15 on triple-MRA. For observer 1 there was complete agreement between DSA and triple-MRA regarding the identification of the main feeding artery. Observer 2 identified the main feeding arteries on triple-MRA in 7 of 8 cases. Eleven and fifteen draining veins were identified on DSA by observers 1 and 2, respectively. They both identified 12 draining veins on triple-MRA.
Discussion
Triple-MRA consistently demonstrated/ruled out residual AVMs in patients who had undergone GKR for brain AVMs compared to DSA. The combination of three MRA techniques is shown to be a robust method to avoid false negative results. Triple-MRA provides volumetric and time resolved information of the AVMs and this may enable more accurate Spetzler-Martin grading, particularly in terms of eloquence of the brain regions involved.
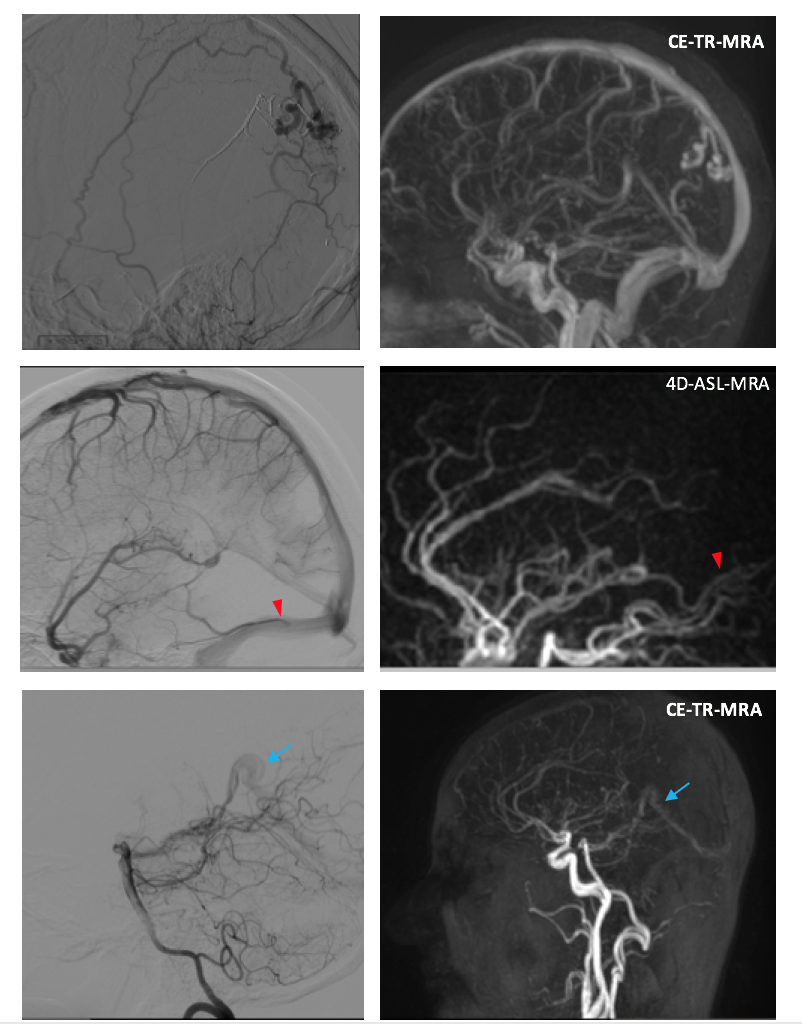
Characterisation of residual AVMs on triple-MRA required assessment of all three MRA techniques (Figure 2). HD-TOF depicts the structural detail of the AVM nidus, 4D-ASL-MRA provides dynamic information of the arterial phase and enables identification of the shunt with modest appreciation of draining veins. CE-TR-MRA better depicts the venous phase.
Conclusions
triple-MRA can be used as an alternative to DSA for confirmation of obliteration of brain AVMs following GKR and for characterisation of residual lesions in cases of incomplete response.Acknowledgements
No acknowledgement found.References
1. Koltz MT, Polifka AJ, Saltos A, Slawson RG, Kwok Y, Aldrich EF, et al. Long-term outcome of Gamma Knife stereotactic radiosurgery for arteriovenous malformations graded by the Spetzler-Martin classification. J Neurosurg. 2013;118(1):74-83.
2. Lee CC, Reardon MA, Ball BZ, Chen CJ, Yen CP, Xu Z, et al. The predictive value of magnetic resonance imaging in evaluating intracranial arteriovenous malformation obliteration after stereotactic radiosurgery. J Neurosurg. 2015;123(1):136-44.
3. Kaufmann TJ, Huston J, 3rd, Mandrekar JN, Schleck CD, Thielen KR, Kallmes DF. Complications of diagnostic cerebral angiography: evaluation of 19,826 consecutive patients. Radiology. 2007;243(3):812-9.
Figures