2449
4D Flow MRI analysis of cerebral blood flow before and after EC-IC bypass surgery1Radiology, Nippon Medical School, Tokyo, Japan, 2Radiology, Nihon University School of Medicine, Tokyo, Japan, 3Healthcare, Philips Electronics Japan, Tokyo, Japan
Synopsis
The purpose of this study was to demonstrate the feasibility of 4D Flow MRI to monitor the change of flow dynamics between before and after extracranial-intracranial (EC-IC) bypass surgery. We enrolled 14 patients who underwent EC-IC bypass. In all, 5 patients underwent radial artery graft (RAG) bypass and 9 patients underwent superficial temporal artery (STA) bypass. All patients underwent 4D Flow MRI preoperatively and 3 weeks after surgery. We measured blood flow volume (BFV) of bilateral internal carotid artery (ICA), basilar artery (BA), and EC-IC bypass artery using 4D flow MRI. Post/pre-operative BFV ratio of contralateral ICA was statistically higher in patients with the RAG bypass group than in those with the STA bypass group (1.28±0.26 in RAG bypass group vs 0.94±0.14 in STA bypass group, p<0.01). 4D Flow MRI could assess comprehensive flow dynamics of EC-IC bypass surgery. It is feasible to clarify the change of contribution from each artery.
Introduction
Extracranial-intracranial (EC-IC) bypass is an option in carefully selected patients with ischemic cerebrovascular disease and a complex intracranial aneurysm, although its use remains controversial. After EC-IC bypass surgery, each intracranial artery (i.e. internal carotid artery (ICA) and basilar artery (BA)) and bypass artery is supposed to supply blood flow complementarily to satisfy the demand of entire brain tissue. In the previous study, the cerebral flow in the patients with post bypass surgery was evaluated by time-resolved 3D phase contrast (4D Flow) MRI which could acquire entire blood flow data in one acquisition with wide coverage [1]. However, in the study, 4D Flow MRI was performed only at a single time point not over time. The purpose of this study was to demonstrate the feasibility of 4D Flow MRI to monitor the change of flow dynamics between before and after EC-IC bypass surgery.Materials and methods
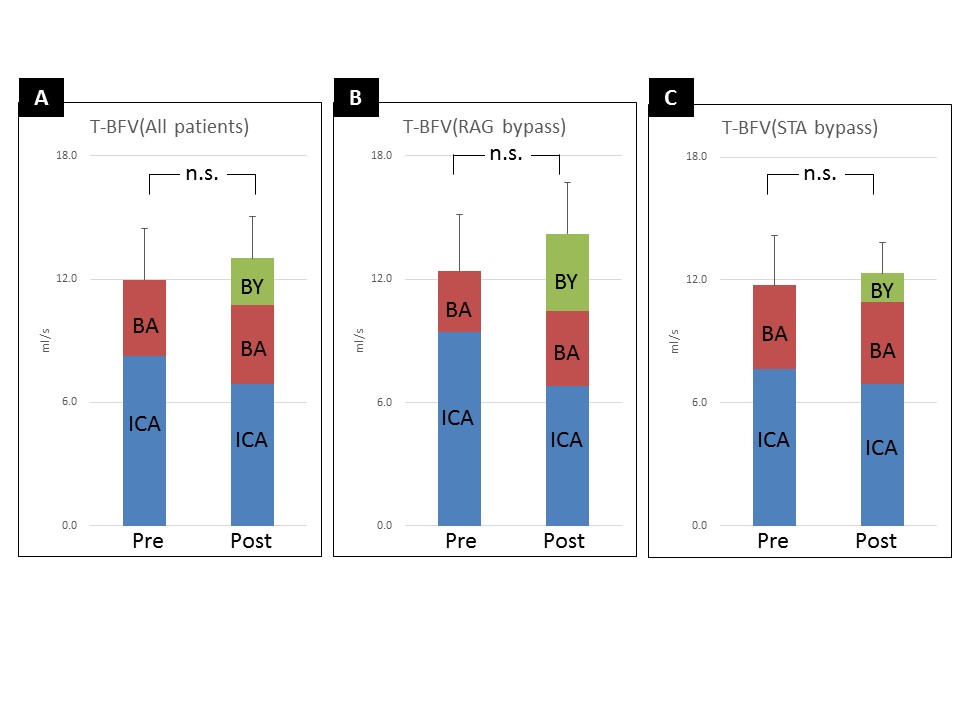
We enrolled 14 patients who underwent EC-IC bypass (5 men, 9 women; mean age at surgery 63.5 years, range 41–81 years). In all, 5 patients underwent ICA ligation and radial artery graft (RAG) bypass surgery for treatment of a complex aneurysm. The other 9 patients with internal carotid artery stenosis (ICS) or occlusion (ICO) underwent superficial temporal artery (STA) bypass surgery. In all patients, 4D Flow MRI were performed preoperatively and 3 weeks after bypass surgery using an Achieva 3.0-T MRI unit with eight-channel head coil (Philips Medical Systems, Best, The Netherlands). The imaging parameters of 4D Flow MRI were as follows; TR/TE=8.4/5.4, FA=13, FOV=210X210X49mm, VENC=100cm/sec, voxel size=0.82X0.82X1.4mm, heart phase= 15. The combined acceleration techniques were as follows; SENSE (factor=2), view sharing with retrospective triggering (k-space segmentation factor was modified depending on heart rate to meat enough actual phase percentage (> 70%)), elliptical k-space coverage (phase-slice direction). As a result, scan time was approximately 6 minutes to meet clinical workflow. The flow volume data were generated from a 4D Flow MRI data set using GT Flow software (GyroTools, Zurich, Switzerland). We measured blood flow volume (BFV) of bilateral ICA, BA, and bypass artery. BFV of each vessel and total brain blood flow volume (t-BFV = bilateral ICA + BA + bypass) were compared before and after surgery by using paired t-test. We also compared post/pre-operative BFV ratio between RAG bypass group and STA bypass group using Student’s t-test.Results
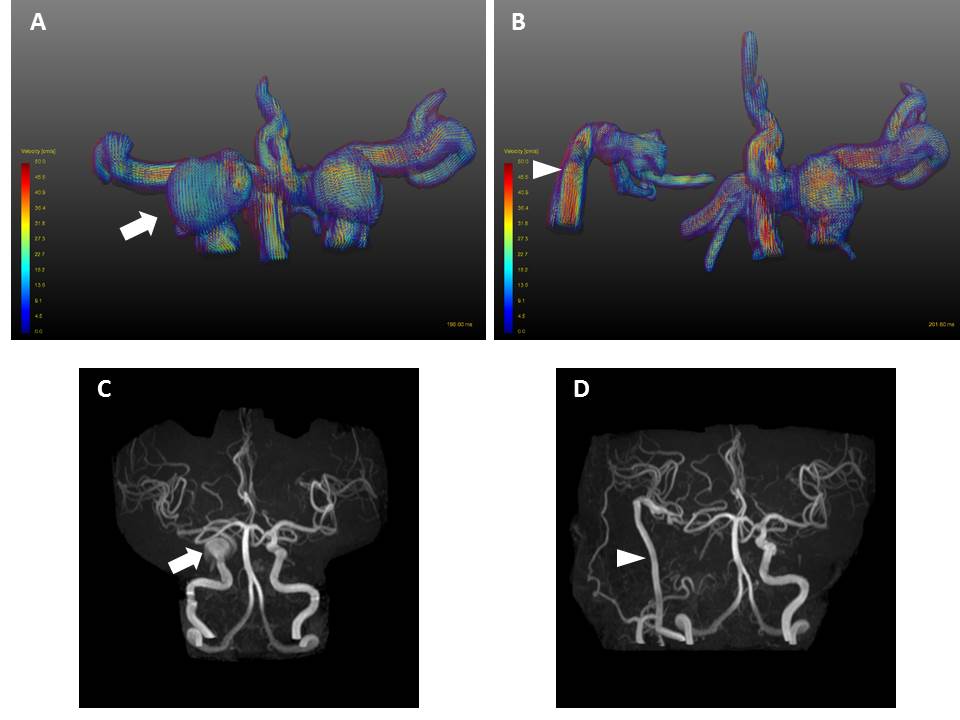
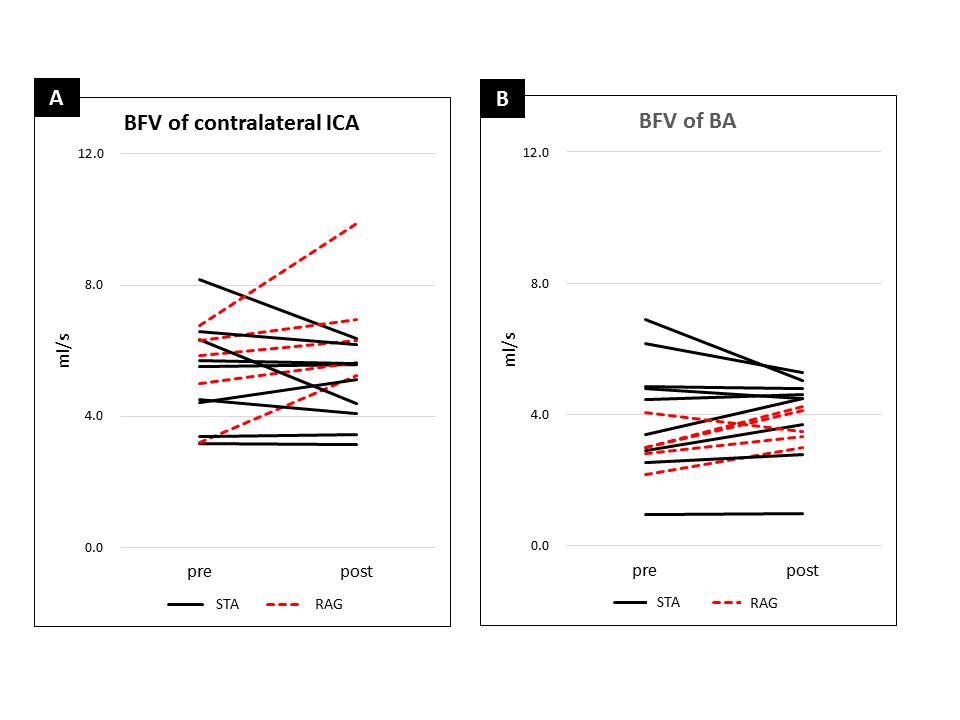
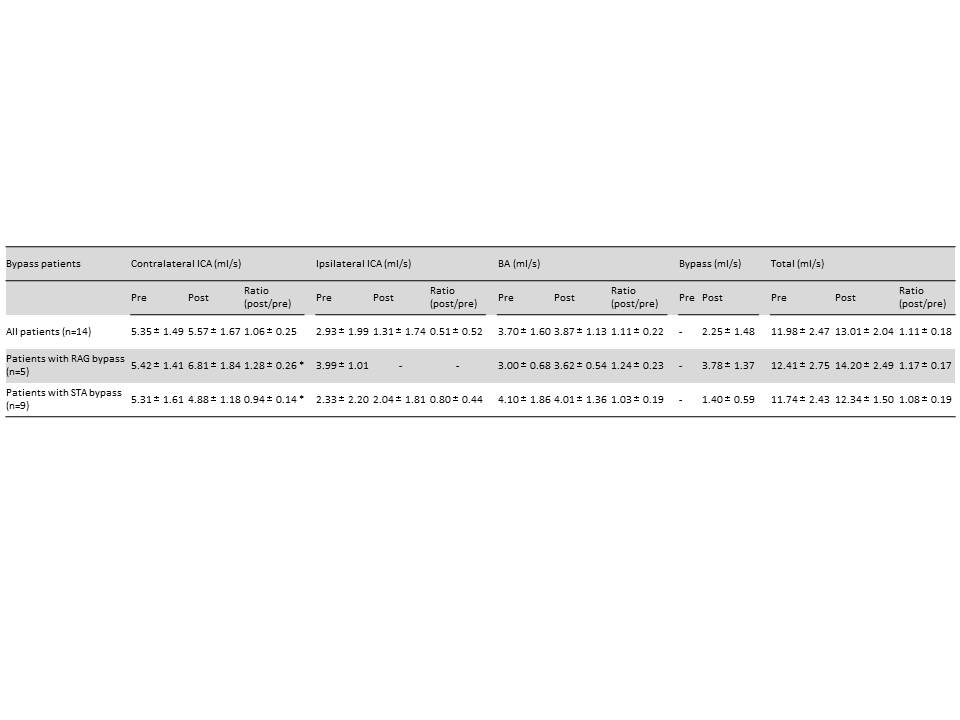
Representative case is shown in Figure 1. Results of the BFV analysis are summarized in Figures 2, 3 and 4. Post/pre-operative BFV ratio of contralateral ICA was statistically higher in patients with the RAG bypass group than in those with the STA bypass group (1.28±0.26 in RAG bypass group vs 0.94±0.14 in STA bypass group, p<0.01). While, no statistical difference was observed in the ratio of BA (1.24±0.23 in RAG bypass group vs 1.03±0.19 in STA bypass group) (Fig. 4).Discussion
This study revealed that 4D Flow MRI could assess comprehensive flow information quantitatively, especially in the post-operative change of the contribution from each artery. In RAG bypass group, the ligation of the large artery (ipsilateral ICA) leads crucial change for flow dynamics. Not only the bypass artery but contralateral ICA and BA compensated the decreased BFV from sacrificed ICA (post/pre ratio; contralateral ICA 1.28±0.26, BA 1.24±0.23, respectively.). In STA bypass group, the complementary flow from STA-bypass had subtle impact on contralateral ICA or BA (post/pre ratio; contralateral ICA 1.06±0.25, BA 1.11±0.22, respectively).
The limitation of this study are as below. First, we only have small patient size which could impact on statistical power. Second, three weeks might be too early to assess post-operative change. Further longitudinal follow up by 4D Flow MRI is needed. Third, the collateral pathway of Willis ring (i.e. anterior and posterior communicating artery) was not assessed. They could affect the change of flow dynamics. Fourth, we didn’t focus on the clinical aspects, the prediction of bypass failure or recurrent stroke.
Conclusion
4D Flow MRI could assess comprehensive flow dynamics before and after EC-IC bypass surgery. It is feasible to clarify the change of contribution from each artery.Acknowledgements
None.References
[1] Sekine T. 4D flow MRI assessment of extracranial-intracranial bypass: qualitative and quantitative evaluation of the hemodynamics. Neuroradiology 2016;58:237-244.Figures