2444
Acceleration-selective Arterial Spin Labeling (AccASL) MR Angiography of Brain Arteriovenous Malformation1Clinical Radiology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan, 2Philips Electronics Japan, Tokyo, Japan
Synopsis
In the present study, we demonstrated the clinical utility of acceleration-selective arterial spin labeling (AccASL) MR angiography (MRA) in brain arteriovenous malformations (AVMs). AccASL-MRA significantly improved the visualization of AVM in comparison with time-of-flight (TOF)-MRA. AccASL-MRA could detect the nidus and draining veins in all patients. In particular, the detection of deep venous drainage by AccASL-MRA led to the accurate Spetzler-Martin grading. AccASL-MRA could serve as a noninvasive tool to evaluate brain AVMs without the use of contrast agents.
Purpose
Brain arteriovenous malformation (AVM) is a congenital vascular disorder characterized by a nidus forming the transition between the feeding artery and draining vein which can cause a serious intracranial hemorrhage. MRI plays a crucial role in detection, diagnosis and grading of brain AVM; However, the visualization of AVM by non-contrast enhanced time-of-flight (TOF) MR angiography (MRA) is limited compared to other methods using contrast agents such as contrast enhanced MRA, CT angiography and digital subtraction angiography (DSA). The vessel visualization in TOF MRA largely depends on the inflow effect of unsaturated blood spins into an imaging slab in the feet-to-head direction. This set-up is thus not optimal for visualizing blood flow that is not in the feet-to-head direction, complex or slow flow. Consequently, TOF MRA frequently fails to depict brain AVMs.
Recently, a gradient design for selective labeling of arterial blood was proposed where the effective gradient form is such that the first moment (m1) is zero. This gradient wave form results in rephasing of the signal of spins moving from constant velocity. The signal from spins that are subject to acceleration will be dephased. As the pulsatile arterial flow has a major acceleration component, whereas venous flow is mostly constant, only arterial blood spins will be visualized. This approach is called acceleration-selective arterial spin labeling (AccASL)1, 2. Previously we demonstrated that AccASL-based MRA enabled better efficiency for visualizing cerebral arteries compared to the TOF-MRA, while suppressing cortical vein signal in normal volunteers3 and patients with Moyamoya disease4. In this study, we evaluated the utility of AccASL-MRA in depiction of brain AVM.
Methods:
[Patients] Sixteen patients with brain AVMs (age 27.0 ± 20.5 year-old; 7 males, 9 females) were examined. All patients underwent both MRA and DSA within an interval of 3 months.
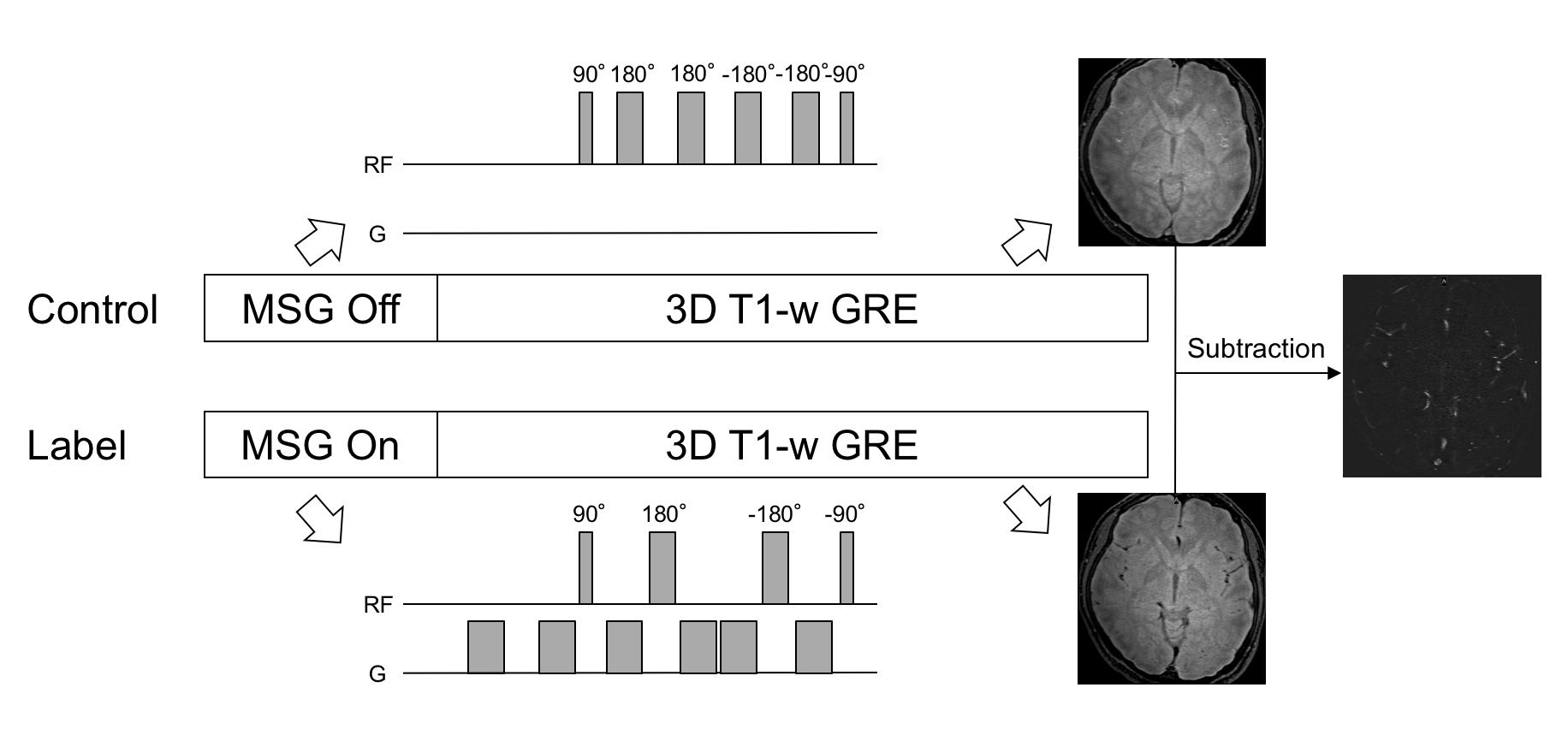
[MRI] Both TOF- and AccASL-MRA were performed on a 3T MR scanner (Ingenia3.0CX, Philips). The AccASL-MRA consists of control (T2-preparation without motion-sensitized gradient: MSG) and label (with MSG) parts followed by 3D T1-weighted gradient-echo sequence (Figure 1). In the label part, MSG employs a motion compensation design to selectively detect spins with acceleration component in arteries. The AccASL acquisition parameters were: sequence T1-TFE; TR/TE, 7.5/3.5 ms; flip angle, 11°; turbo factor, 60; shot interval (sequence TR), 1500 ms; 3D slab thickness, 120 mm; voxel size, 0.39×0.77×1.0 mm (120 partitions); SENSE factor, 2.0; and total acquisition time for the label and control pair of 6min9sec. The TOF-MRA was obtained in the identical imaging resolution, geometry and acquisition time as AccASL-MRA.
[Image Analysis] The following matters are compared between AccASL- and TOF-MRA using the DSA findings as a reference standard; 1, detection rate; 2, size of nidus; 3, venous drainage pattern; 4, Spetzler-Martin grade; 5, visualization; 6, contrast-to-noise ratio (CNR). Visualization of each component of AVM was evaluated with 5-points grading scale. CNR of each component was evaluated in 3-5 regions on 20 mm-thick partial MIP images with the following equation; CNR = (Vesselmax – WMave) / WMSD
[Statistical Analysis] The detection rate, size of nidus, visualization, and CNR were compared between the two MRA methods by Fisher’s exact test, paired t-test, Wilcoxon matched paired test, and paired t-test, respectively.
Results
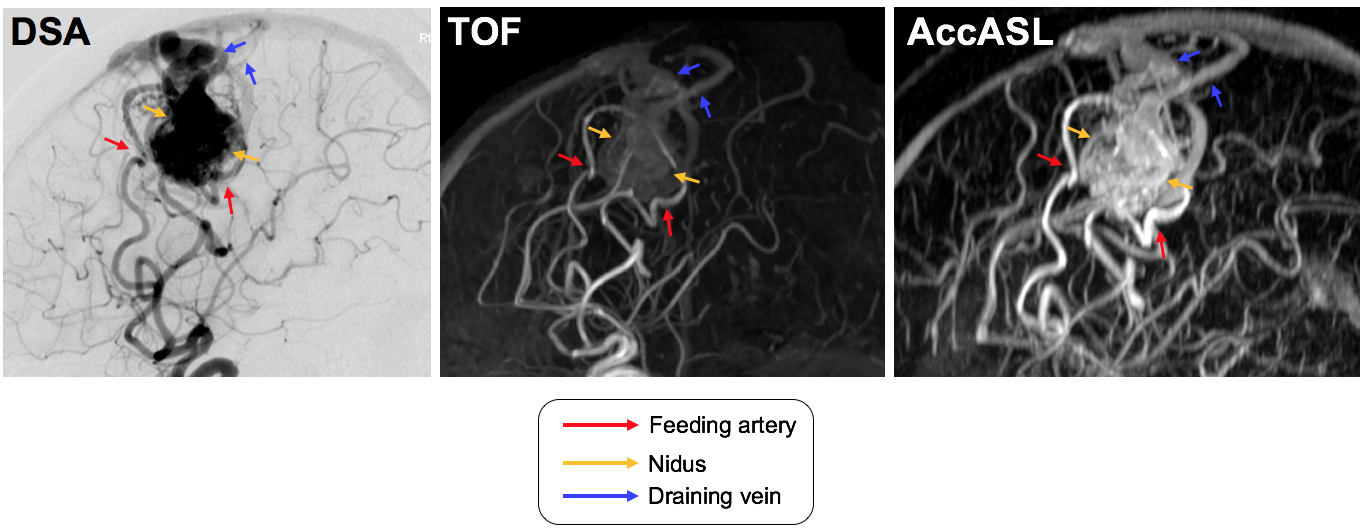
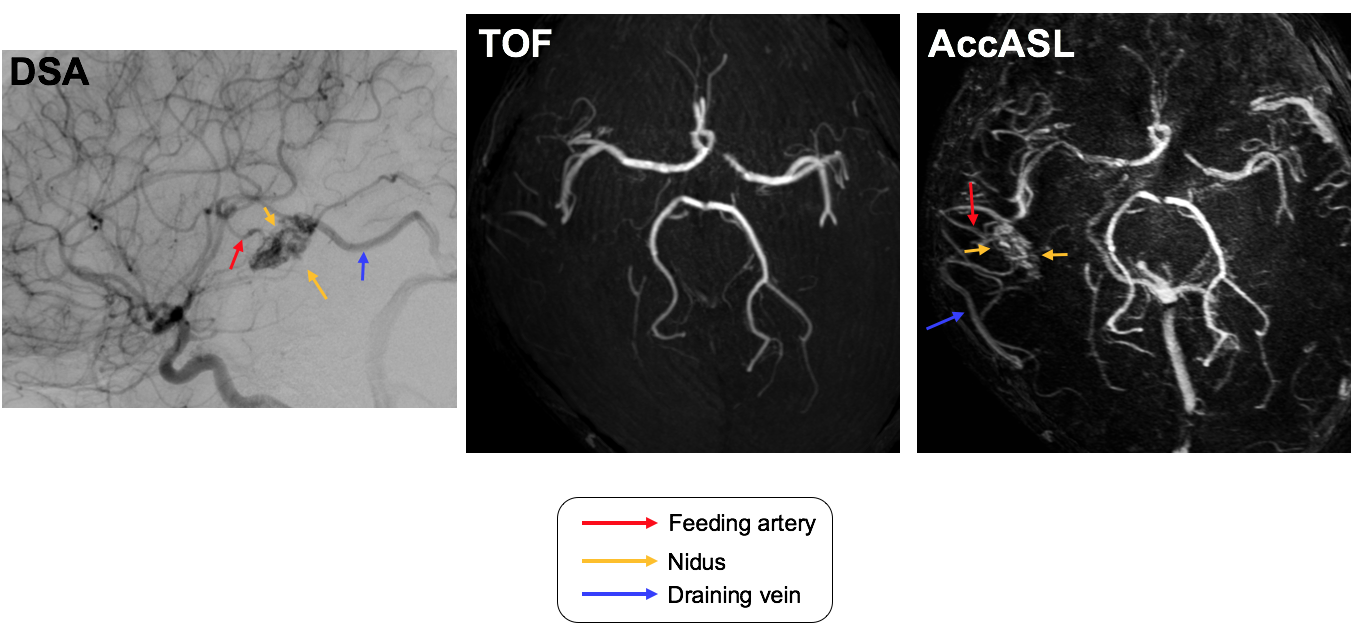
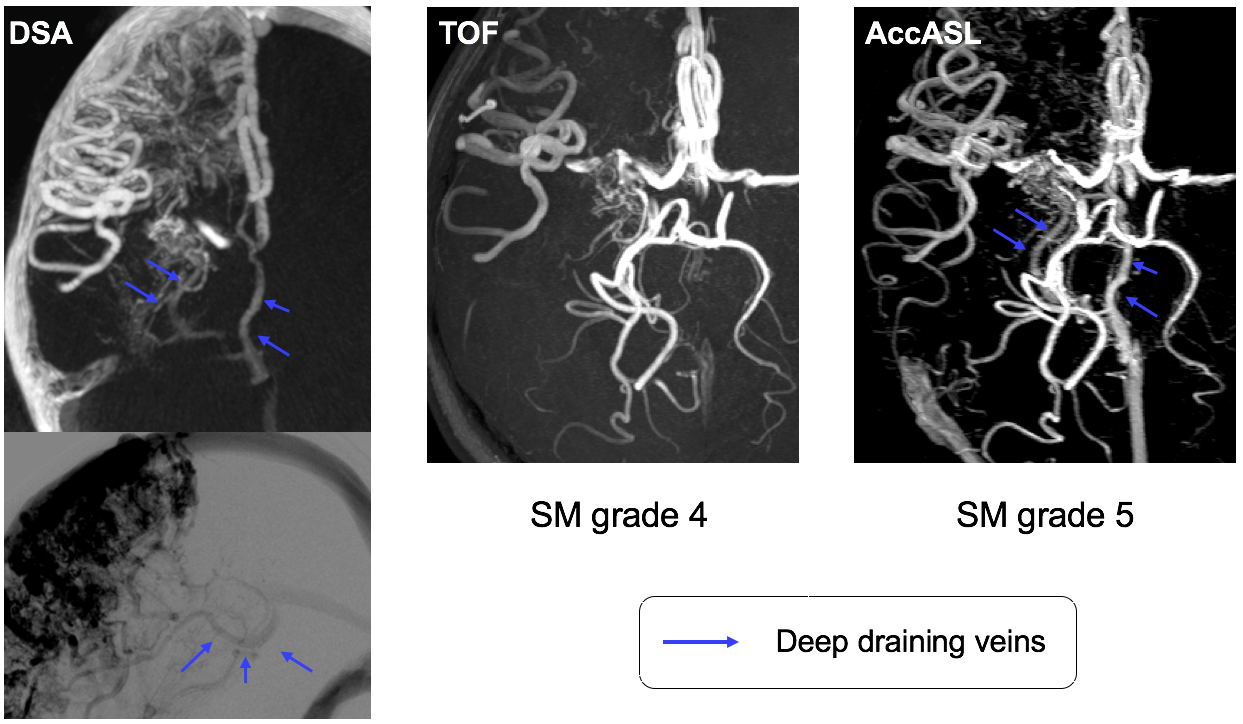
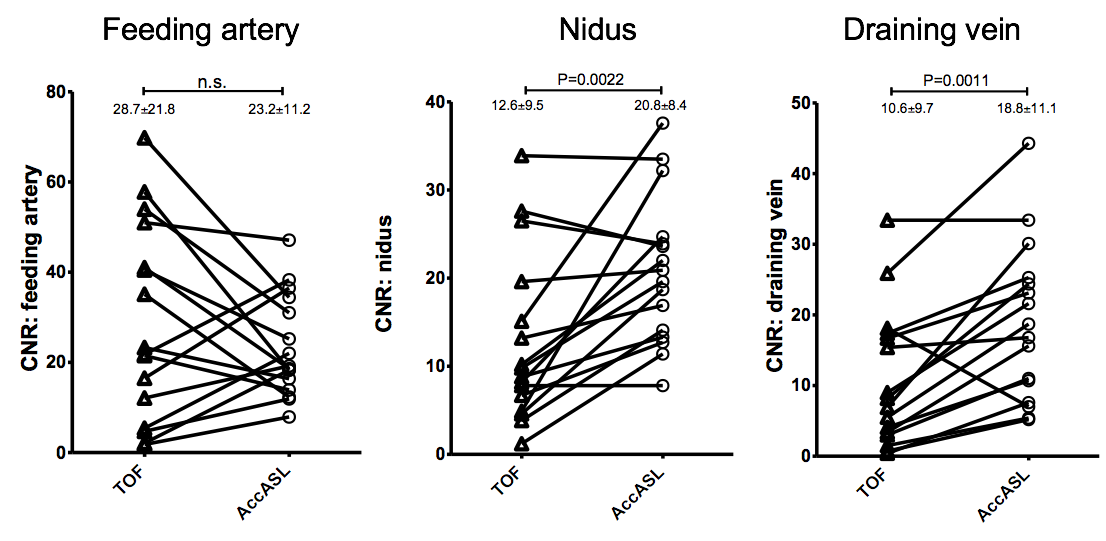
Figure 2 shows a representative case of brain AVM where AccASL-MRA shows better visualization of the nidus and draining veins. TOF-MRA detected AVMs in 11 out of 16 patients (68%) while AccASL detected in all patients (100%, P<0.05, Figure 3). The size of nidus did not differ between the two MRA methods. TOF-MRA failed to depict deep venous drainage in 4 patients which resulted in the underestimation of Spetzler-Martin grade whereas AccASL could accurately assess venous drainage pattern and Spetzler-Martin grade in all patients (Figure 4). The visualization scores for nidus (TOF: 2.8±1.6, AccASL: 4.7±0.9, P<0.0001) and draining vein (TOF: 2.8±1.5, AccASL: 4.4±1.2, P<0.001) were higher with AccASL-MRA than with TOF-MRA while those for feeding artery (TOF: 4.0±1.5, AccASL: 4.7±0.8) were not different between the methods. The CNRs of nidus (TOF: 12.6±9.5, AccASL: 20.8±8.4, P<0.01) and draining vein (TOF: 10.6±9.7, AccASL: 18.8±11.1, P=0.001) were higher with AccASL-MRA than with TOF-MRA while those of feeding artery (TOF: 28.7±21.8, AccASL: 23.2±11.2) were not different between the methods (Figure 5).Discussion
Our present findings demonstrated the potential of AccASL-MRA in visualizing complex and multi-directional flow in a nidus, which was limited in TOF-MRA. AccASL was sensitive enough to identify slow deep venous drainage typically in the head-to-feet direction. AccASL-MRA can be a clinical tool which enables us to detect, diagnose and grade brain AVMs.Conclusion
AccASL-MRA improved the visualization of a nidus and draining vein in AVM. AccASL-MRA could serve as a noninvasive tool to evaluate brain AVMs without the use of contrast agents.Acknowledgements
No acknowledgement foundReferences
1. Priest AN, Taviani V, Graves MJ, Lomas DJ. Improved artery-vein separation with acceleration-dependent preparation for non-contrast-enhanced magnetic resonance angiography. Magn Reson Med. 2014;72(3):699-706.
2. Schmid S, Ghariq E, Teeuwisse WM, Webb A, van Osch MJ. Acceleration-selective arterial spin labeling. Magn Reson Med. 2014;71(1):191-9.
3. Obara M, Togao O, Yoneyama M, et al. Acceleration-selective arterial spin labeling for intracranial MR angiography with improved visualization of cortical arteries and suppression of cortical veins. Magn Reson Med. 2016.
4. Togao O, Hiwatashi A, Obara M, et al. Acceleration-selective arterial spin Labeling (AccASL) MR angiography for visualization of distal cerebral arteries in Moyamoya disease. Proceedings of the 24th annual meeting of the international society of magnetic resonance in medicine. Singapore 2016
Figures