2443
Detection of cerebral microvascular lesions using 7 T MRI in patients with neuropsychiatric systemic lupus erythematosus1Division of Pulmonary Medicine,Allergy,and Rhematology,Department of internal Medicine, Iwate Medical University, morioka, Japan, 2Pulmonary Medicine,Allergy,and Rheumatology, Iwate Medical University, Morioka, Japan, 3Ultra-High Field MRI and Department of Radiology, Iwate Medical University, morioka, Japan
Synopsis
We investigated whether high-resolution images obtained using ultrahigh field MRI at 7 T can detect microcerebrovascular lesions in patients with neuropsychiatric systemic lupus erythematosus (NPSLE) that have never been detected by conventional MRI. We prospectively examined 20 patients with SLE, including five with NPSLE, using a 7 T MRI scanner. On the high-resolution T1WIs obtained at 7 T, minute punctate/linear hyperintense lesions in subcortical and/or cortical areas were found in four (80%) NPSLE patients and one (7%) non-NPSLE patient. High-resolution T1WIs obtained at 7 T can detect minute lesions, indicating intracerebral microvascular lesions in patients with NPSLE.
Purpose
Systemic lupus erythematosus (SLE) is a multisystemic autoimmune disease of unknown etiology. The clinical manifestations of SLE show mucocutaneous, articular, renal, serosal, hematologic, and immunologic involvement. Among the manifestations, neuropsychiatric SLE (NPSLE) is one of the most common causes of morbidity and mortality among patients with SLE. No acceptable methods for diagnosing NPSLE have been established. Conventional MRI of the brain has been thought to be a useful tool for understanding the etiologic processes of NPSLE. However, whether these MRI findings are related to the symptoms of NPSLE remains unclear. The absence of MRI findings in NPSLE cases could potentially be attributed to a low power field of magnetic resonance and the low-resolution capacity of conventional MRI. Therefore, we analyzed the CNS lesions of patients with NPSLE using 7 T MRI in the present study.Methods
Subjects
We recruited 20 consecutive patients with SLE. All patients fulfilled the 1982 revised criteria for the lassification of SLE. The patients with NPSLE were diagnosed by a board-certified rheumatologist (N.S.) as well as board-certified neurologists and psychiatrists according to the 1999 case definitions for NPSLE syndromes.
Imaging protocol
MRI examination was conducted using a 7T scanner (Discovery MR950; GE Healthcare, Milwaukee, Wisconsin, USA) with a 32-channel head coil. T1-weighted images (T1WIs) before and after the administration of contrast agent (0.1mmol/kg gadopentetate dimeglumine; Bayer AG, Leverkusen, Germany) were obtained. T1W images, TR 12ms, TE 2.8ms, flip angle 12°, FOV 200 mm, matrix size 512×320 (pixel size 0.4×0.6mm), slice thickness 0.5mm (after zero-fill interpolation), number of slices 170, and acquisition time 9min 35s.
Results
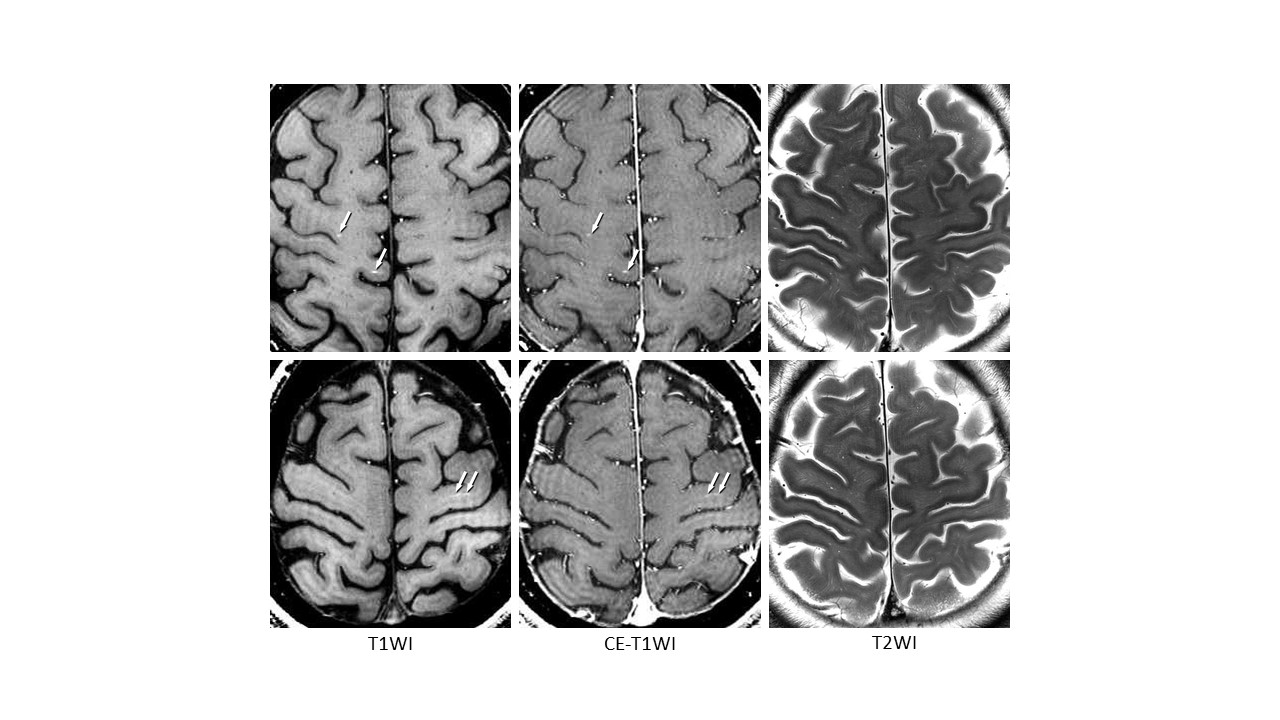
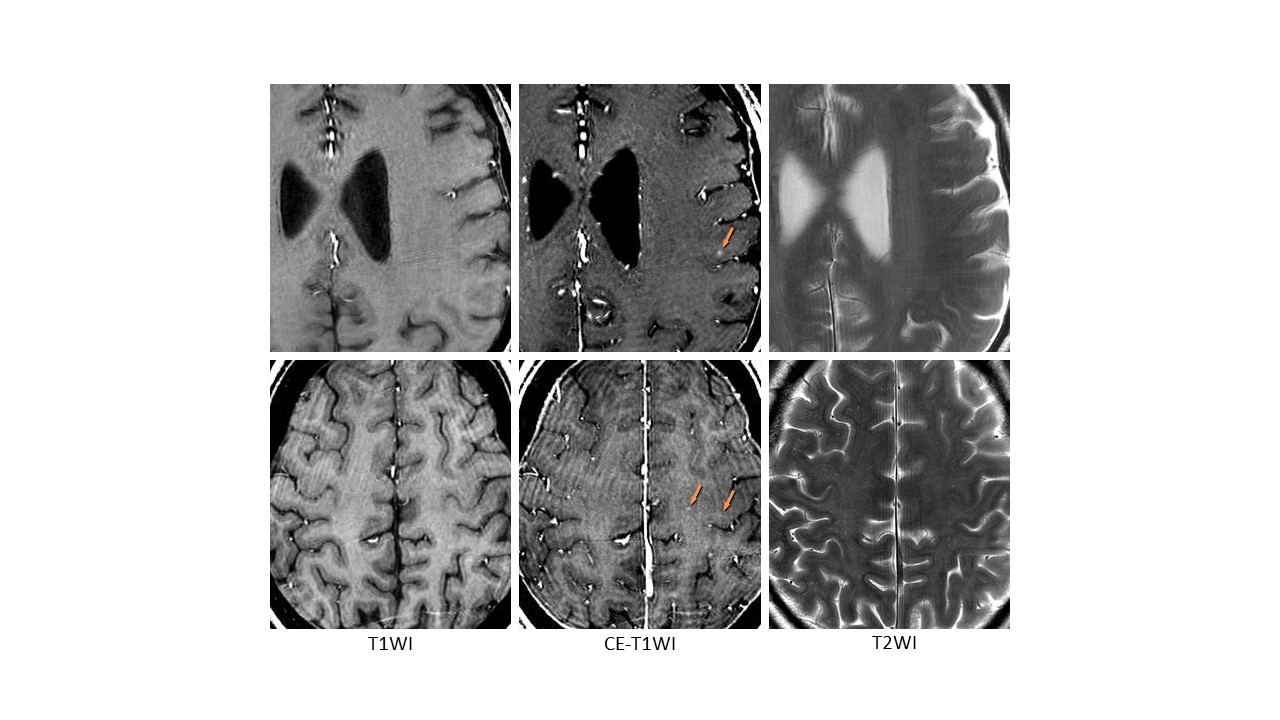
Among the 20 patients with SLE, five were diagnosed with NPSLE. The symptoms of the patients with NPSLE included polyneuropathy (one patient), acute state of confusion (two), psychosis (one), cognitive dysfunction (one), and ischemic stroke (two). All of the patients underwent MRI examinations and all the resulting images were eligible for further analyses. On the high-resolution T1WIs, minute punctate and/or linear hyperintense lesions, subcortical/cortical microhyperintensities (SCMH), were found in the subcortical and/or cortical areas of the cerebral hemisphere, particularly in high-convexity areas, in four of five patients with NPSLE (80%) and one of 15 patients with non-NPSLE (7%). In addition, on high-resolution T1WIs obtained after the administration of the contrast agent, punctate enhanced lesions, subcortical/cortical microenhancement (SCME), were only found in these areas in three NPSLE patients (60%), with some lesions showing hyperintensity and others being unclear on the non-enhanced T1WIs. These lesions were significantly more frequent in the NPSLE patients compared with the non-NPSLE patients. No abnormal signals were found in the corresponding areas on the high-resolution T2WIs. In addition to these lesions, findings indicating an old infarct including a hemorrhagic infarct were reported in one NPSLE patient (20%, thalamus and cerebellum) and three non-NPSLE patients (20%, cerebral deep white matter and basal ganglia). Nonspecific deep white matter hyperintensities were found in one (20%) NPSLE patient and four (27%) non-NPSLE patients.Discussion
The present study suggests that SCMH and SCME on 7TMRI images might be indicative of early lesions that are not detected by conventional MRI and may serve as useful indices to diagnose NPSLE. The pathogenesis of NPSLE has been thought to involve the impairment of microcirculation in the brain. The early recognition and evaluation of NPSLE is critically important as NPSLE is responsible for 7–13% of deaths from SLE.1 Conventional MRI is valuable in detecting CNS lesion in acute focal NPSLE manifestations. However, detecting the lesions responsible for NPSLE in all cases is difficult. To date, there have been reports of various nonspecific findings in NPSLE patients; however, no CNS findings were detected in NPSLE patients by conventional MRI. Nomura et al. reported that 38 of 100 SLE patients without neurological deficits showed an abnormality in the CNS on 1.0 T MRI. 2 These findings were thought to include subclinical lesions of NPSLE and nonspecific lesions unrelated to the pathogenesis of SLE. In this regard, to prevent deaths from NPSLE, we need to detect the early lesions responsible for NPSLE by distinguishing them from nonspecific findings. The present study demonstrated that SCMH and SCME on T1WIs at 7 T were significantly frequent in the patients with NPSLE compared with non-NPSLE patients.Conclusion
High-resolution T1WIs at 7 T detect minute findings indicative of intracerebral microvascular lesions in patients with NPSLE. MRI at 7 T might therefore be a useful tool to diagnose NPSLE in the early stages.Acknowledgements
This work was partly supported by a Grant-in-Aid for Strategic Medical Science Research (S1491001) from the Ministry of Education, Culture, Sports, Science, and Technology of Japan. O.M. carried out the primary data analysis and wrote the manuscript. N.S. contributed to study design and clinical management. M.S. contributed to study design, interpretation of the results, and writing of the manuscript. K.K., Y.N., Y.O., H.K., and Y.N. helped with data collection of SLE patients. K.Y. contributed to discussion of the results and writing of the manuscript.References
1.Tucker LB, Menon S, Schaller JG, Isenberg DA. Adult- and childhood-onset systemic lupus erythematosus: a comparison of onset, clinical features, serology, and outcome. Br J Rheumatol 1995; 34:866–872.
2. Nomura K, Yamano S, Ikeda Y, Yamada H, Fujimoto T, Minami S, et al. Asymptomatic cerebrovascular lesions detected by magnetic resonance imaging in patients with systemic lupus erythematosus lacking a history of neuropsychiatric events. Intern Med 1999; 38:785–795.
Figures