2406
Inductively coupled coils enable dental MRI with 350 um isotropic resolution in 2 min1Department of Radiology, Medical Physics, Medical Center - University of Freiburg, Freiburg, Germany, 2Faculty of Medicine, University of Freiburg, Freiburg, Germany, 3Division of Oral and Maxillofacial Surgery, Medical Center - University of Freiburg, Freiburg, Germany, 4Partner Site Freiburg, German Consortium for Cancer Research (DKTK), Heidelberg, Germany
Synopsis
High-resolution MRI of the lower jaw with an isotropic voxel size of 350 μm was performed at 3T using a 4-cm loop coil (LC) with and without an inductively coupled volume coil (ICC) enclosing the target region. Within this region, a much higher SNR was obtained and the resolution of anatomical details was strongly enhanced with the ICC. A new, custom-made holder for the LC improved the overall handling. Compared to earlier results, the scan time was reduced by 50%, now 2 minutes, to provide very high resolution MRI of 2-3 teeth.
Introduction
In dentistry, information on both hard tissue (enamel, dentin, cementum and bone) and soft tissue (gingiva, dental pulp, the neurovascular bundle, mucosa, lips and facial tissues) is essential for diagnosis and treatment. Cone beam computed tomography (CBCT) delivers excellent hard tissue contrast, but only poor visualization of soft tissues. Magnetic Resonance Imaging (MRI) has proven to be a valuable alternative 1-3, however, the small size of the structures of interest < 1 cm is a serious challenge for the resolution of conventional MRI. Several approaches to address this challenge were described, including wireless, inductively coupled volume coils 4. Here, we present the latest developments of this technology that allows MRI of a selected volume with an isotropic voxel size of (350μm)3 in less than two minutes. Special focus is laid on shortening the scan time to reduce motion artefacts, improving image quality and patient comfort.
Materials & Methods
Coil Holder
A new setup was designed to improve the work flow of dental MRI measurements (Fig. 1), consisting of variable head fixations and a flexible tube (acetal copolymer, LOC-LINE Flexi, Lockwood Products Inc., Lake Oswego, USA) to accommodate a 4-cm loop coil (LC) both mounted on a custom-made base plate (PVC). For MRI, the head of a volunteer was fixed with cushions in between the plates, and the LC was placed at the desired position (jaw) using the flexible tubes (Fig. 1).
Inductively Coupled Coils
Inductively coupled coils (ICC) were used as described previously 3,4. The resonance frequency of the ICC was adjusted by tuning a variable capacitor and a network analyzer in S11 mode with an untuned 8-cm pick up coil (ZVB4 Vector Network Analyzer, Rhode & Schwarz, Munich, Germany) after placement in vivo. For the same volunteer and the same coil positioning, no retuning was necessary between different imaging sessions.
MRI Experiments
Written informed consent from a male volunteer (27 y) was obtained. All MRI experiments were performed on a 3T clinical whole body scanner equipped with a body transmit coil, a 4-cm receive loop coil (LC), with or without the ICC (MAGNETOM Prisma, Siemens Healthineers, Erlangen, Germany). 3D gradient echo imaging was performed with the following parameters: slice thickness = 0.35 mm, TE/TR = 2.6/7.1 ms, 1 or 2 averages, matrix size = 192x192, BW = 270 Hz/px, α = 15°, in plane resolution = (0.35x0.35) mm2, FOV = (67x67) mm2, acquisition time ~ 2 min, slab selective excitation. For comparison, experiments were performed with and without ICC and otherwise identical imaging parameters (except the number of averages, which was set to 2 for the measurement without ICC, resulting in an acquisition time ~ 4 min).
Results
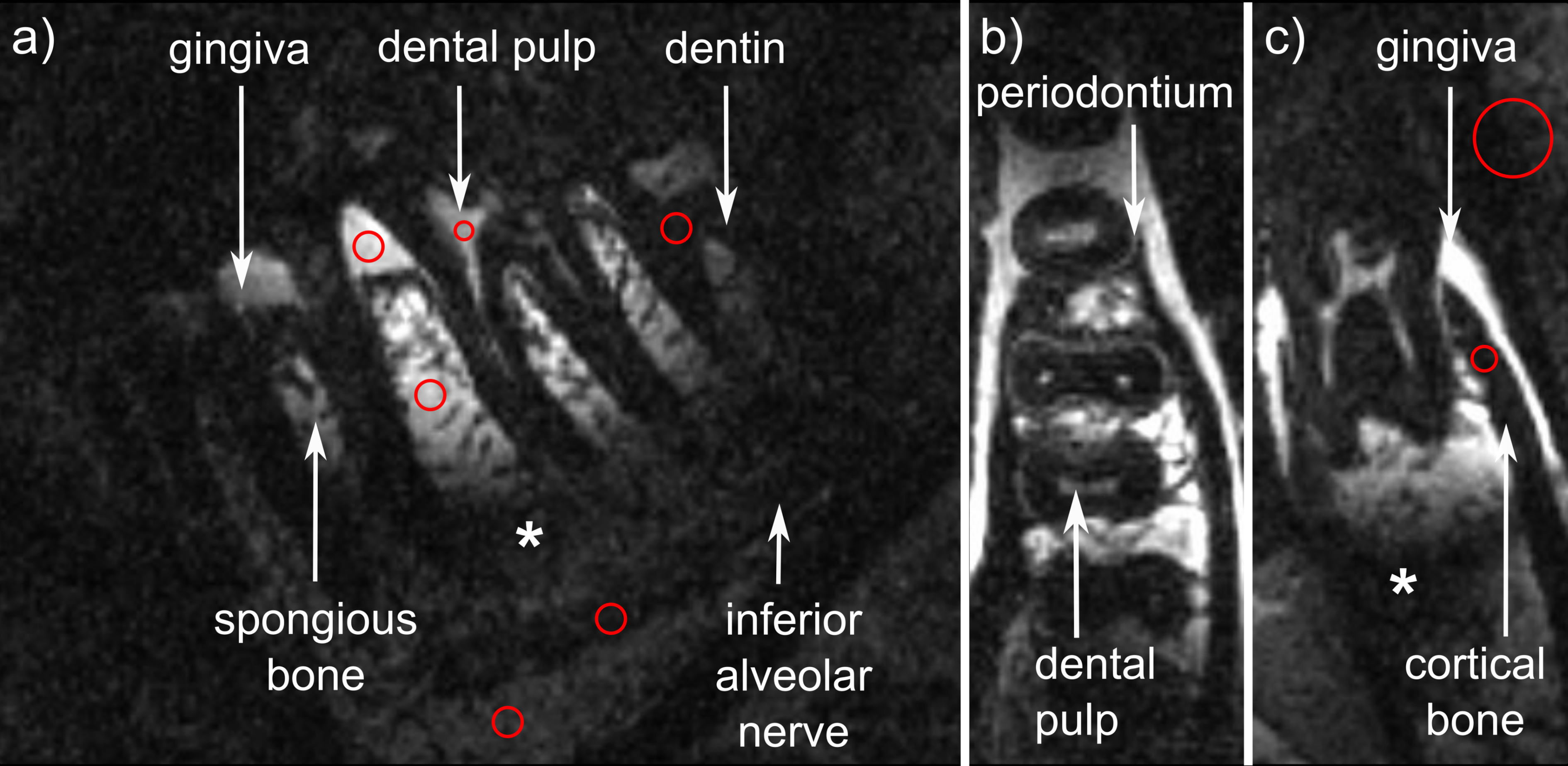
The new setup enabled an easy placement and a stable
positioning of the LC during the MRI examination (Fig. 1). Compared to earlier reports 4, a strong but lower SNR was obtained in
half of the acquisition time with the ICC, and the representation of anatomical
details like the periodontium appeared to be improved (Fig. 2). Some but not all
loss in SNR can be attributed to the fact that one instead of 2 averages were
used (e.g. SNR 41 to 57 4 for interdental gingiva). Like before, a signal
void caused by the ICC geometry was observed in the root region.
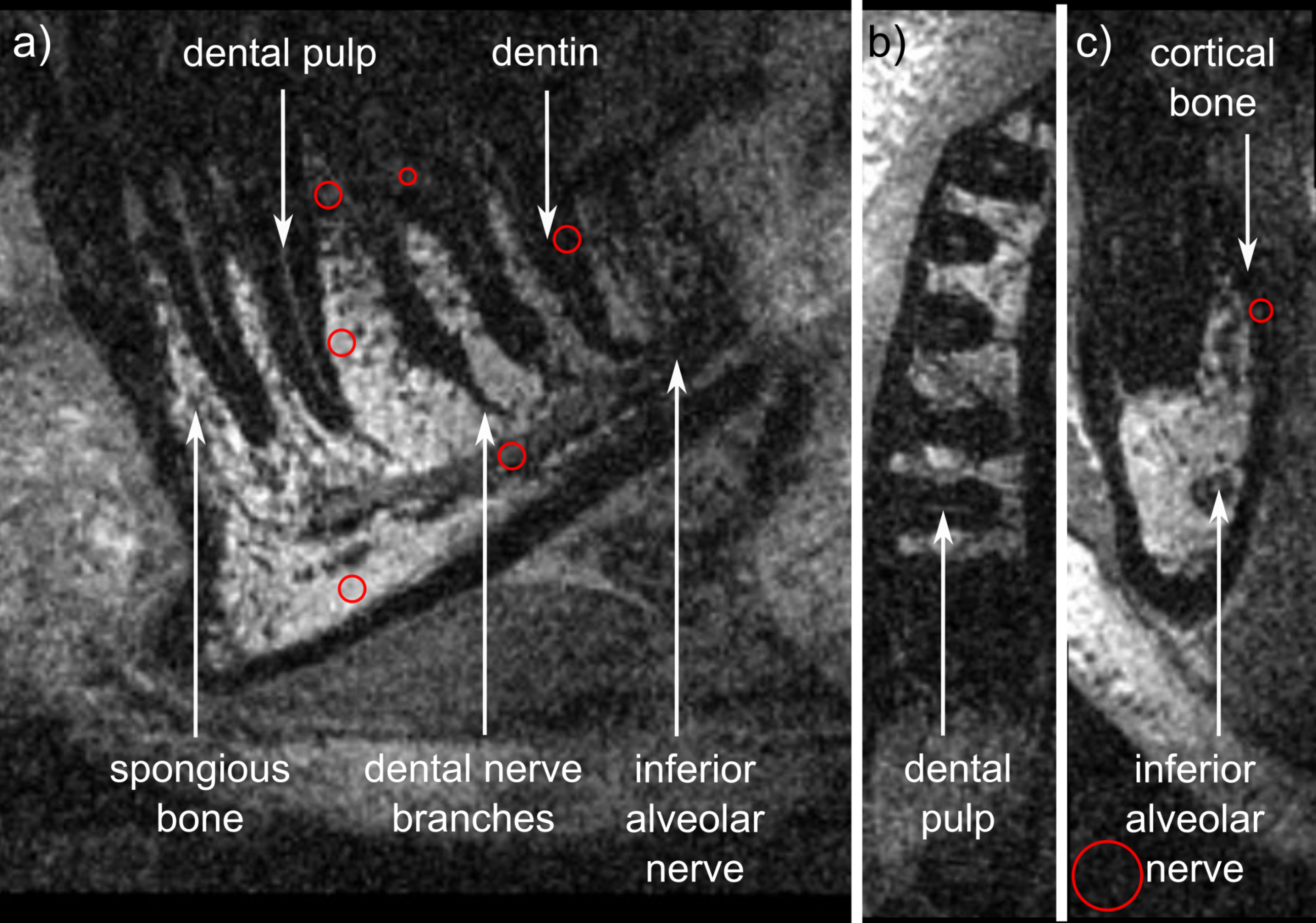
In comparison, the LC alone provided better coverage
of the roots (Fig. 3), clearly displaying the branches of the dental nerves.
However, small structures as the periodontium were not resolved, and SNR
was reduced despite the acquisition of two averages (Tab. 1).
By using the ICC, SNR of selected anatomical
structures was improved, e.g. 8-fold for interdental gingiva (corrected
for different averages, Tab. 1).
Discussion
The newly developed setup improved the overall workflow of the dental MRI examination strongly. Furthermore, and possibly attributed to more precise coil placement and less motion artefacts (subtle blurring), the number of averages (and scan time) was cut in half, while the display of fine anatomical details was retained or improved. Compared to earlier reports, a similar but somewhat lower SNR was observed, which needs to be confirmed in future measurements. The signal void observed between the wires of the ICC remains an issue.Conclusion
Dental MRI with 350 μm isotropic resolution was achieved in half of the scan time than before. This is likely attributed to an improved patient and coil positioning, resulting in less motion artefacts. This technique appears very promising to monitor processes that were previously inaccessible to the limited resolution of conventional MRI, including but not limited to the longitudinal monitoring of bone augmentation or dental vitality.Acknowledgements
Support by the DFG (HO 4604/2-1) and the Osteology Foundation (Switzerland) is acknowledged.References
1. Prager M, Heiland S, Gareis D, Hilgenfeld T, Bendszus M, Gaudino C. Dental MRI using a dedicated RF-coil at 3 Tesla. J Craniomaxillofac Surg 2015;43(10):2175-2182
2. Assaf AT, Zrnc TA, Remus CC, Schönfeld M, Habermann CR, Riecke B, Friedrich RE, Fiehler J, Heiland M, Sedlacik J. Evaluation of four different optimized magnetic-resonance-imaging sequences for visualization of dental and maxillo-mandibular structures at 3 T. J Craniomaxillofac Surg 2014;42:1356-1363
3. Flügge T, Hövener JB, Ludwig U, Eisenbeiss AK, Spittau B, Hennig J, Schmelzeisen R, Nelson K. Magnetic resonance imaging of intraoral hard and soft tissues using an intraoral coil and FLASH sequences. Eur Radiol 2016; Epub ahead of print
4. Ludwig U, Eisenbeiss AK, Scheifele Nelson K, Bock M, Hennig J, von Elverfeldt D, Herdt O, Flügge T, Hövener JB. Dental MRI using wireless intraoral coils. Sci Rep 2012;6:23301
Figures