2394
Neuroimaging in Concussion: A Magnetic Resonance Elastography Pilot Study1Radiology, Mayo Clinic Arizona, Phoenix, AZ, United States, 2Neurology, Mayo Clinic Arizona, Phoenix, AZ, United States, 3Mayo Clinic Rochester, Rochester, MN, United States, 4Research, Mayo Clinic Arizona, Phoenix, AZ, United States
Synopsis
As concussion, even when symptomatic, can be occult on routine imaging, there is clinical need for a more accurate diagnostic assessment. The objective of this study was to assess the utility of brain magnetic resonance elastography (MRE), a non-invasive neuroimaging technique, to detect changes in brain stiffness in concussed patients relative to healthy controls.
Introduction
Over 2 million people are diagnosed with a concussion each year, with approximately 300,000 concussions resulting from sports-related activities alone [1]. The consequences of concussion due to post-concussion symptoms, treatment side effects, and the resulting disability, place a staggering burden on society. According to the most recent guidelines [2], a concussion is defined as an event caused by a sudden blow to the head or other parts of the body resulting in concomitant short-term disturbances of physical, cognitive and emotional functioning. Although symptoms generally resolve over the course of a few days, about 15% of concussed patients have persistent symptoms for at least 3 months after the concussive event [3]. Although concussion can manifest with a myriad of short-term and long-term symptoms of varying severity, routine diagnostic imaging is typically unable to detect anatomical abnormalities associated with concussion [4,5]. This disconnect between clinical symptoms and lack of neuroimaging findings causes a dilemma for making accurate clinical diagnoses, for prognosticating recovery, and for establishing return-to play guidelines. The objective of this study is to assess the utility of brain magnetic resonance elastography (MRE) to detect changes in brain stiffness in concussed patients relative to healthy controls.Method and Materials
Three concussion patients and three age- and gender-matched healthy controls were included in this study with IRB approval and written consent. The MRE studies were performed on a 3T GE scanner (Discovery 750w, General Electric, Milwaukee, WI) using a modified 2D spin echo EPI (SE-EPI) pulse sequence with 3D motion sensitizing gradients. A novel passive driver and an eight-channel head coil were used for all cases. An operating frequency of 60 Hz was chosen to apply to all the subjects. MRE images were acquired after obtaining high resolution 3D T1-weighted images to ensure proper brain coverage and to provide a clear brain tissue comparison structure. The MRI protocol included 3D T1 FSPGR (TR/TE/TI/voxel size/slices/FA/matrix = 8.4/3.7/450/0.85x0.85x1.0/160/20/256x256) and MRE (TR/TE/TI/voxel size/slices/FA/matrix = 3600/70/na/3x3x3/49/90/72x72). An atlas in the MNI space was used for automatically identifying different structures, such as left and right frontal, parietal and temporal lobes. The T1-weighted images were first registered to the MRE magnitude Images. The atlas for each region was then transformed to the space of the T1-weighted images. ROIs were then defined based on the atlas of each region and the median absolute shear modulus (|G*|), storage modulus (G’), and a loss modulus (G”) were calculated for each ROI.Results
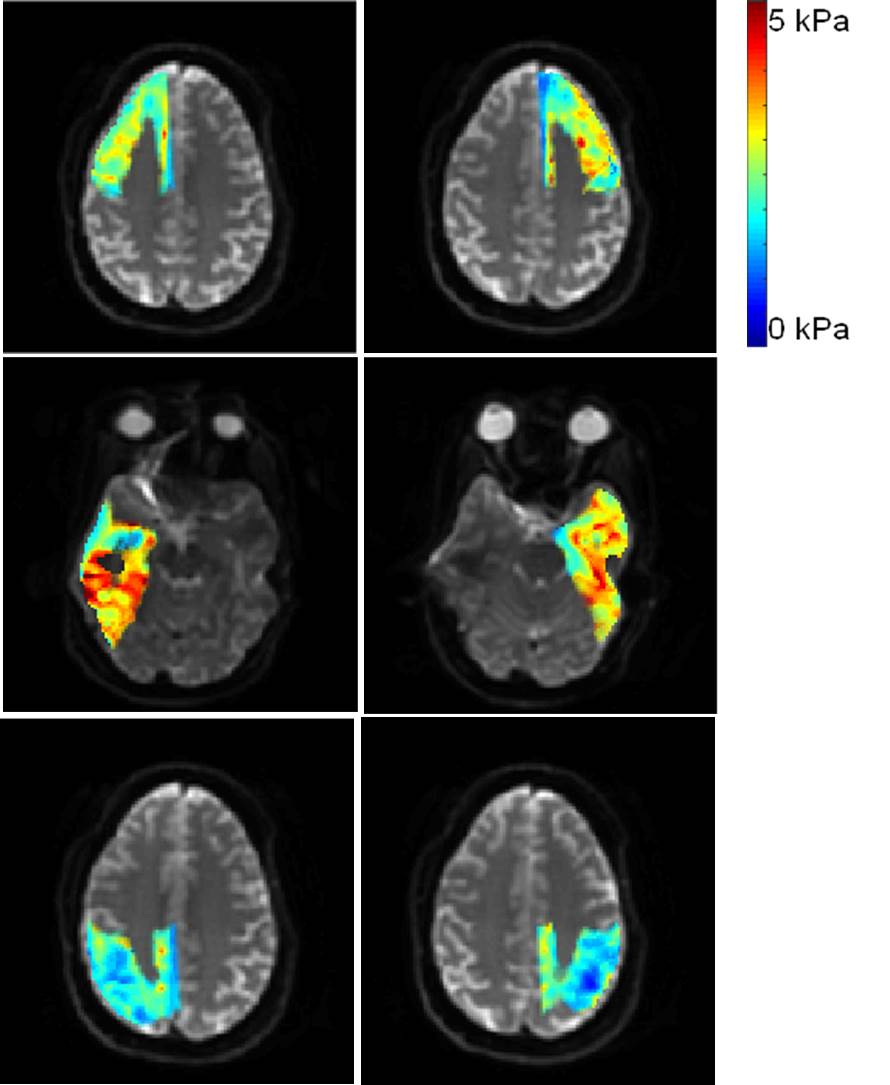
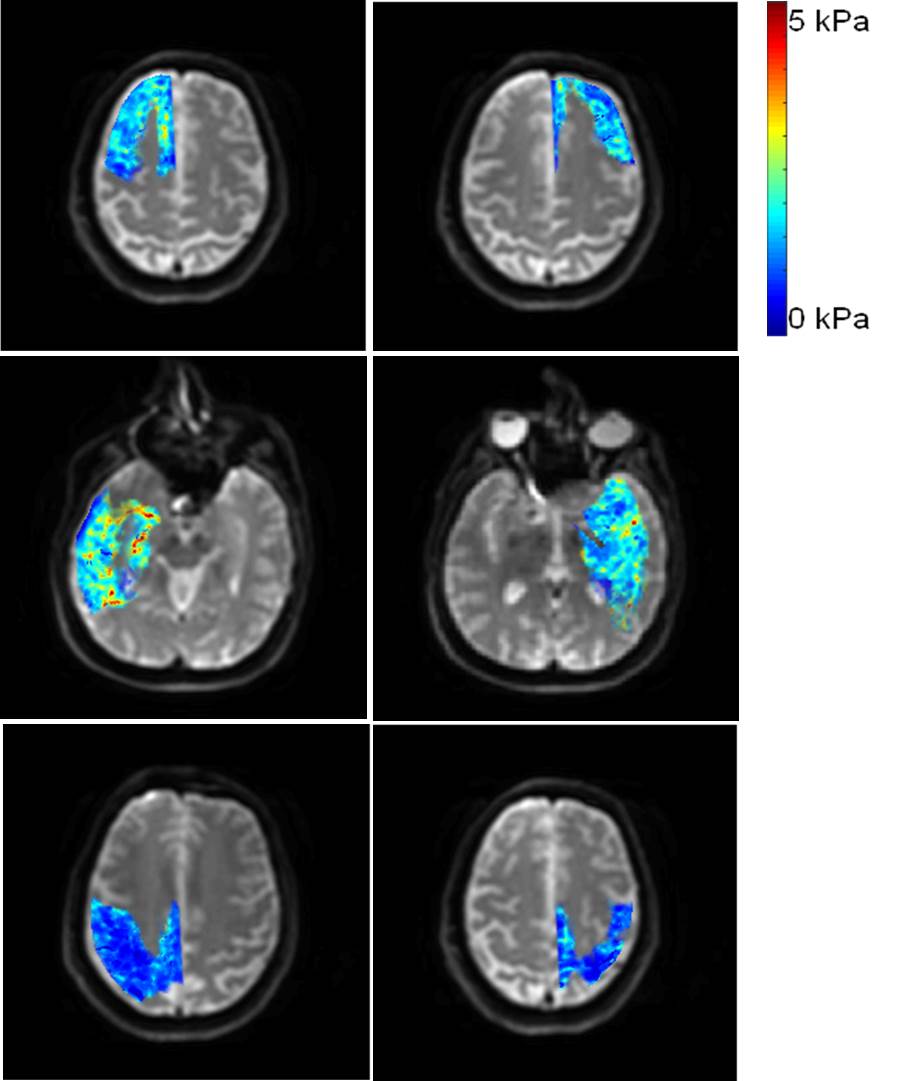
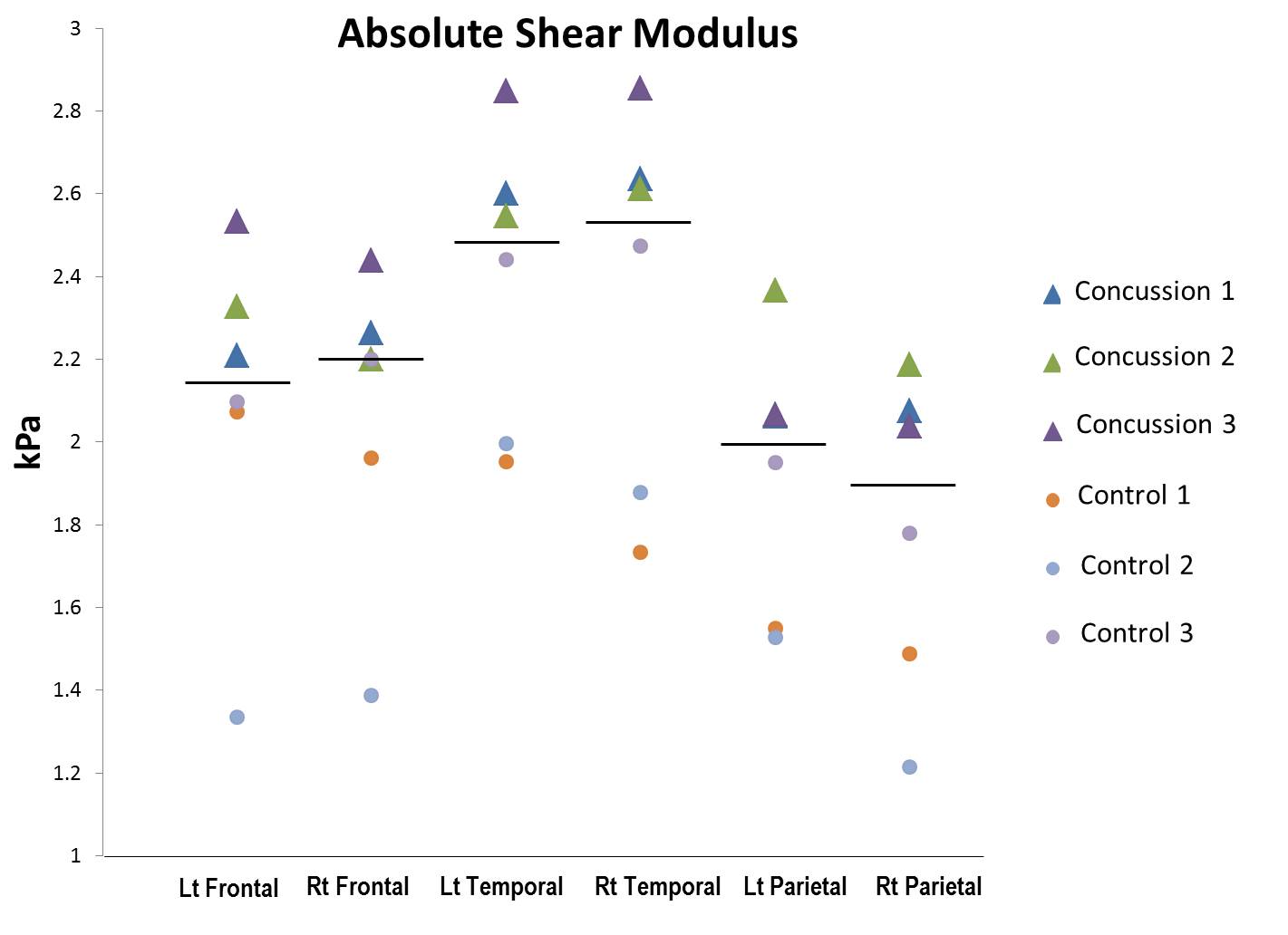
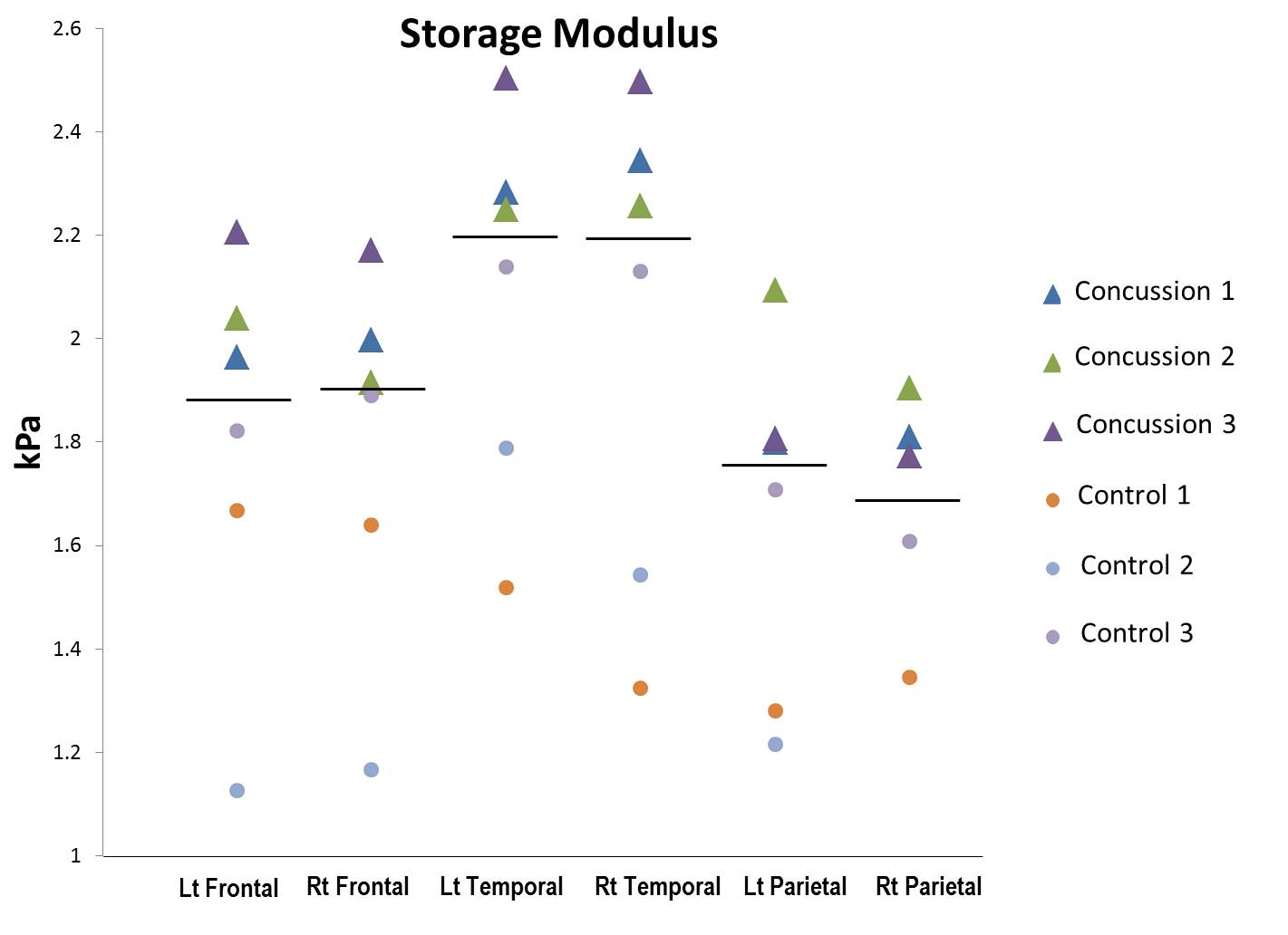
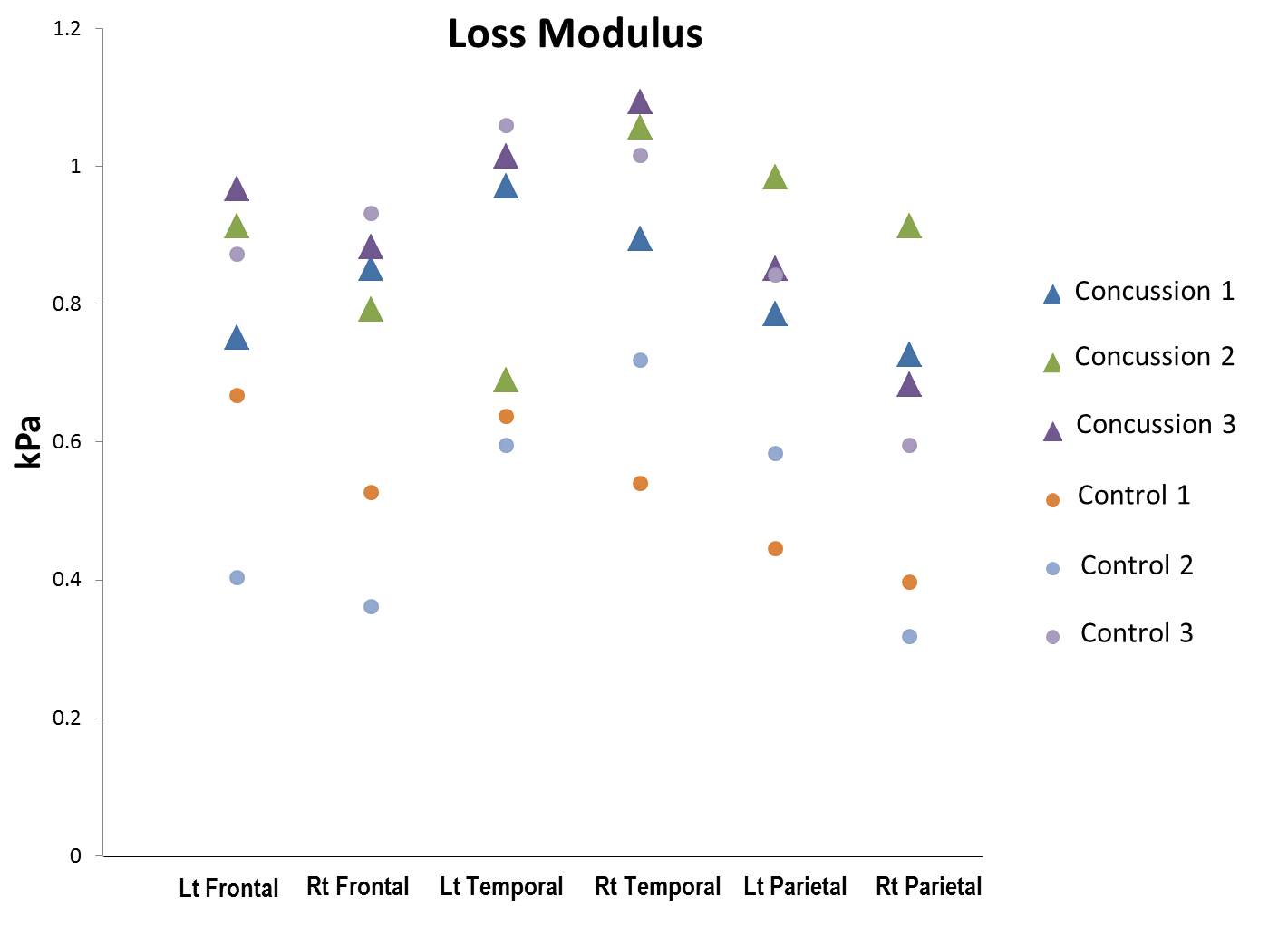
There was relative increased stiffness in all six segmented brain regions (left and right frontal, temporal and parietal lobes) for patients with concussion (Fig 1) as compared to normal controls (Fig 2). Individually plotted values for the absolute shear modulus (Fig 3) and storage modulus (Fig 4) showed the highest stiffness values in the temporal lobes, with clear separation between concussed patients and controls for all lobes except the right frontal. However, the plotted loss modulus values showed generally lower stiffness scores for both concussed patients and controls, with overlap between the two groups (Fig 5).Discussion
Magnetic Resonance Elastography (MRE) has shown to be of utility in detecting changes in the biomechanical properties of the brain related to age and sex [6]; neurological disorders such as normal pressure hydrocephalus [7]; and neuro-degenerative diseases such as dementia [8]. However, to our knowledge, its utility in concussion has not been investigated as of yet. This pilot study suggests that there are global increased brain stiffness changes in patients with concussive symptoms that can be detected with MRE. However, further refinements are likely needed as there are regional variations in the separation of median absolute shear modulus (|G*|) stiffness values across the various brain segments. In addition, the results from this small cohort suggest that the storage modulus (G’; related to elasticity) may be a better biomechanical parameter than the loss modulus (G”; related to viscosity) for discriminating sequelae of concussion from unaffected brain. However, larger studies will be required for this determination.Conclusion
As routine diagnostic imaging is typically unable to detect anatomical sequela associated with concussion, MR Elastography has the potential to noninvasively detect abnormalities in brain elasticity that could serve as an objective biomarker for: a) correlating with the extent of brain damage and recovery; and b) facilitating the accurate clinical diagnosis and prognostication of patients with concussion.Acknowledgements
No acknowledgement found.References
1. Faul M, Xu L, Wald M and Coronado V. Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations, and Deaths, 2002-2006. Atlanta: Centers for Disease Control and Prevention 2010.
2. McCrory P, Meeuwisse WH, Aubry M, et al. Consensus Statement on Concussion in Sport: The 4th International Conference on Concussion in Sport, Zurich, November 2012. Journal of Athletic Training. 2013; 48: 554-75.
3. Shenton ME, Hamoda HM, Schneiderman JS, et al. A review of magnetic resonance imaging and diffusion tensor imaging findings in mild traumatic brain injury. Brain imaging and behavior. 2012; 6: 137-92.
4. Binder LM. A review of mild head trauma. Part II: Clinical implications. J Clin Exp Neuropsychol. 1997; 19: 432-57.
5. Borg J, Holm L, Cassidy JD, et al. Diagnostic procedures in mild traumatic brain injury: results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J Rehabil Med. 2004: 61-75.
6. Arani A, Murphy MC, Glaser KJ, Manduca A, Lake DS, Kruse SA, Jack CR Jr, Ehman RL, Huston J 3rd. Measuring the effects of aging and sex on regional brain stiffness with MR elastography in healthy older adults. Neuroimage. 2015 May 1;111:59-64.
7. Huston J 3rd, Murphy MC, Boeve BF, Fattahi N, Arani A, Glaser KJ, Manduca A, Jones DT, Ehman RL.Magnetic resonance elastography of frontotemporal dementia. J Magn Reson Imaging. 2016 Feb;43(2):474-8.
8. Fattahi N, Arani A, Perry A, Meyer F, Manduca A, Glaser K, Senjem ML, Ehman RL, Huston J. MR Elastography Demonstrates Increased Brain Stiffness in Normal Pressure Hydrocephalus. AJNR Am J Neuroradiol. 2016 Mar;37(3):462-7.
Figures