2383
Thalamic Atrophy following mTBI is Associated with Persistent Post-Concussive Symptoms and Cognitive Fatigue1Diagnostic Radiology and Nuclear Medicine, University of Maryland School of Medicine, Baltimore, MD, United States, 2Electrical and Computer Engineering, Johns Hopkins University
Synopsis
Even mild TBI patients with negative CT and MRI may experience persistent post-concussive symptoms (PCS) and declined cognition more than 3 months post injury. In this prospective study of regional brain volume changes in mTBI patients, we found progressive thalamic atrophy from acute to chronic stages post injury, especially within the patient group that showed persistent PCS at 6 months. Thalamic volume atrophy also correlated with cognitive fatigue and processing speed within the same symptomatic mTBI group. Further studies on vulnerability of the thalamus may provide more insights into TBI recovery and lead to potential Therapies.
Introduction
More than 70% of all TBI patients are in the mild category. Although they often have negative imaging findings from CT and conventional MRI, a significant portion (~40%) experience persistent post-concussive symptoms (PCS) and declined cognition more than 3 months post injury1. In this prospective study we analyze the 3D volumetric MRI data to study regional brain volume changes in mTBI patients and examine their relationship to their post concussive symptoms and neuropsychological assessments.Methods
MRIs on 42mTBI patients (age: 38.2±14.7, 10F/32M) and 42 healthy controls (age: 36.6±14.3, 18F/24M) were acquired on 3T Siemens Trio scanner. Each patient underwent MRI evaluation at acute (<10 days) and chronic (6 months) stages post injury, when both the Rivermead post-concussion symptom Questionnaire2 and Automated Neuropsychological Assessment Metrics (ANAM)3 were administrated. Based on presence of PCS at the chronic stage, the mTBI patients were further divided into the PCS+ (N=20, age: 42.6±14.7, 7F/13M) and PCS- (N=20, age: 34.5±14.0, 3F/19M) groups, based on whether they have presence (self-report rating > 0) of three of more of following symptoms: headaches, dizziness, sleep, trouble concentrating, fatigue, memory problems, and irritability last longer than three months following injury.4 MRI imaging included high resolution T1-weighted MPRAGE sequence acquired with TE/TR=2.91ms/2300ms, TI=900ms, flip angle=9⁰, FOV=256mm, resolution = 1×1×1 mm3. FreeSurfer was used for subcortical segmentation of brain regions, where the regional volumes were extracted.Results
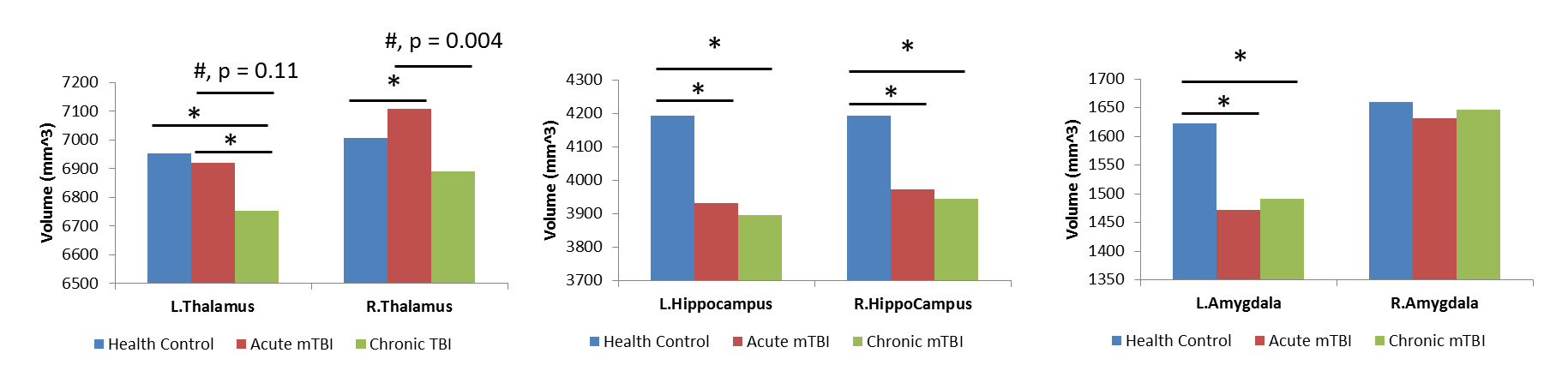
Significantly reduced brain volumes
were observed in mTBI as compared to controls in hippocampus and amygdala
(p<0.05) at both visits, and in the thalamus at the chronic stage.
Paired t-test indicated longitudinal volume atrophy from acute to chronic
stages in the thalamus mTBI patients (p<0.05) (Figure 1).
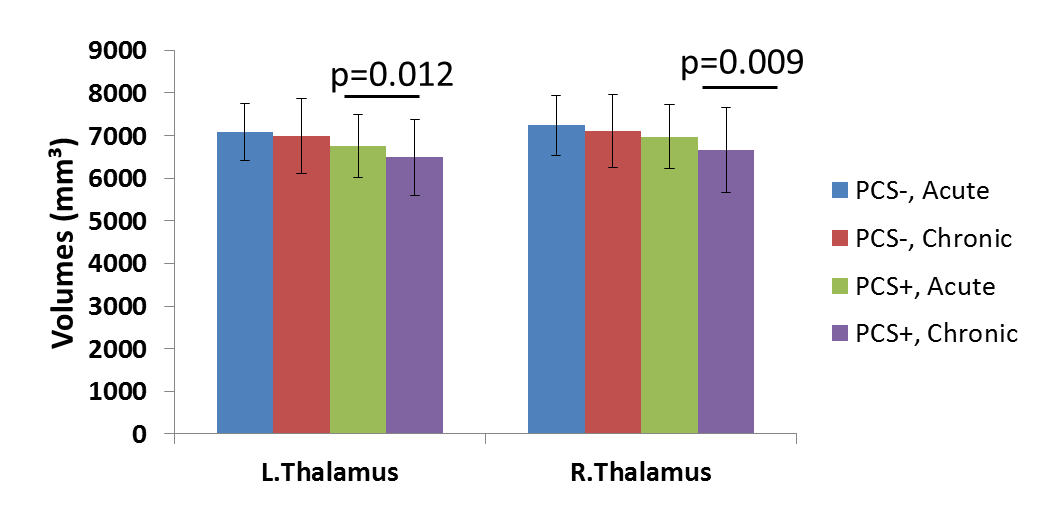
When further divided to PCS+ and PCS- groups, volume atrophy was only
significant in the bilateral thalamus and left pallidum in the PCS+ group but
not in the PCS- group (Figure 2). Within the PCS+ group after adjusting for age
factor, thalamic volume atrophy was further found to correlate with ANAM
subtest that is reflective of cognitive fatigue and processing speed (simple
reaction test repeat) (Left: r = 0.54, p = 0.015; Right: r = 0.476, p = 0.034).Discussion
In this study we found subtle brain volume atrophy as early as within 10 days in mTBI patients in hippocampus and amygdala. While thalamus volume was not significantly reduced acutely, thalamus underwent progressive atrophy over time, especially within the patient group that showed persistent PCS at 6 months. Thalamic volume atrophy also correlated with cognitive fatigue and processing speed within the same symptomatic mTBI group. Further studies on vulnerability of the thalamus may provide more insights into TBI recovery and lead to potential Therapies.Acknowledgements
No acknowledgement found.References
[1] Centers for Disease Control and Prevention. Report to congress on mild traumatic brain injury in the united states: Steps to prevent a serious public health problem. Center for Disease Control. Atlanta, GA. 2003.
[2] King NS, Crawford S, Wenden FJ, Moss NE, Wade DT. The rivermead post concussion symptoms questionnaire: A measure of symptoms commonly experienced after head injury and its reliability. J Neurol. 1995;242: 587–592.
[3] Kane RL, Roebuck-Spencer T, Short P, Kabat M, Wilken J. Identifying and monitoring cognitive deficits in clinical populations using automated neuropsychological assessment metrics (ANAM) tests. Arch Clin Neuropsychol. 2007;22 Suppl 1: S115–26.
[4] World Health Organization. International Classification of Disease. World Health Organization; 2010. 10th Review.
Figures