2364
Racial differences in cerebral microcirculatory function and cognitive function1Department of Radiology and Imaging Sciences, Emory University School of Medicine, Atlanta, GA, United States, 2Department of Medicine, Emory University School of Medicine, Atlanta, GA, United States
Synopsis
We examined racial differences in cerebrovascular reactivity (CVR) to carbon dioxide and their associations with cognitive function among patients with mild cognitive impairment and hypertension. The results provide evidence for association between impaired CVR and executive dysfunction. Hypertensive African Americans have more compromised cerebral microcirculatory function compared to Caucasians.
Introduction
Cerebrovascular reactivity (CVR) to carbon dioxide, a measure of microcirculatory function in the brain, is impaired in hypertension 1 and might be related to poor cognitive performance 2. African Americans (AA) are at double the risk of developing Alzheimer’s disease and age-related cognitive decline 3. In this study, we aimed to evaluate racial differences in CVR and their associations with cognitive function in older adults with mild cognitive impairment (MCI) and hypertension.Methods
Seventy patients (age = 65.16 ± 7.18; 38 females; 45 AA) were included in a clinical trial at baseline visit. All participants had their antihypertensive medicine stopped, underwent cognitive assessment (Montreal Cognitive Assessment (MOCA) score = 21.97 ± 3.22). A 6-minute blood oxygenation level-dependent (BOLD) imaging was acquired by using a gradient-echo EPI sequence: TR/TE = 2500/27 ms, FA = 90°, FOV = 220 x 220 mm2, matrix = 74 x 74, slice-thickness = 3 mm, 48 slices. At 2 minutes after the initiation of the scan, air with increased CO2 concentration (8%) was supplied for 2 minutes. Twenty volumes acquired before and during CO2 inhalation were averaged, respectively. Voxel-based CVR was calculated as percentage augmentation between the 2 stages (baseline and CO2 challenge). CVR maps were then normalized to Montreal Neurological Institute standard space. Regional CVR values were calculated from ROIs of frontal, parietal, temporal and occipital lobes. Associations with cognitive function, including Trail-Making Test Part B (TMTB) and MOCA, were assessed using Person’s correlation. Racial and gender differences were assessed using two-way ANOVA.Results
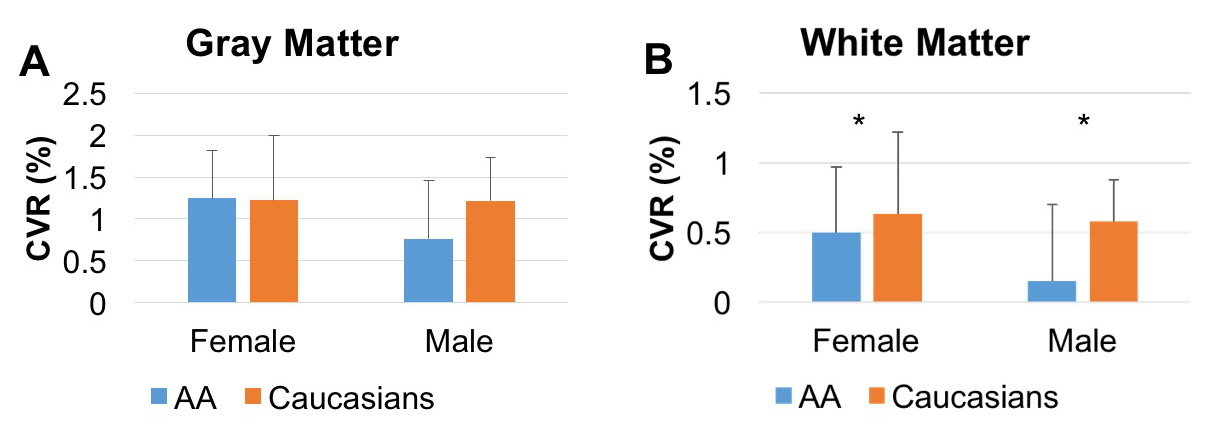
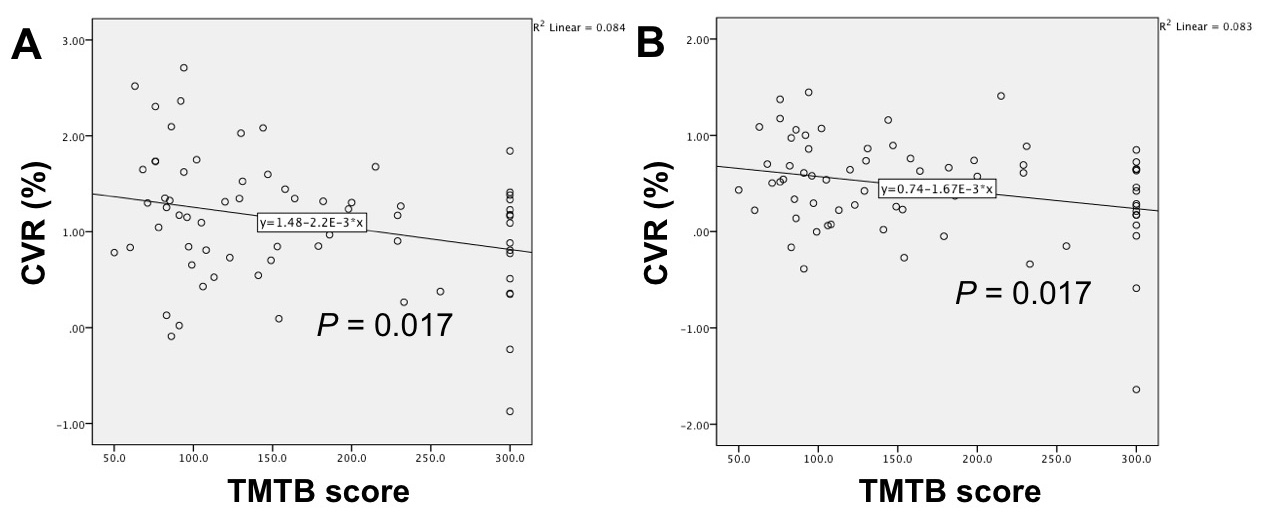
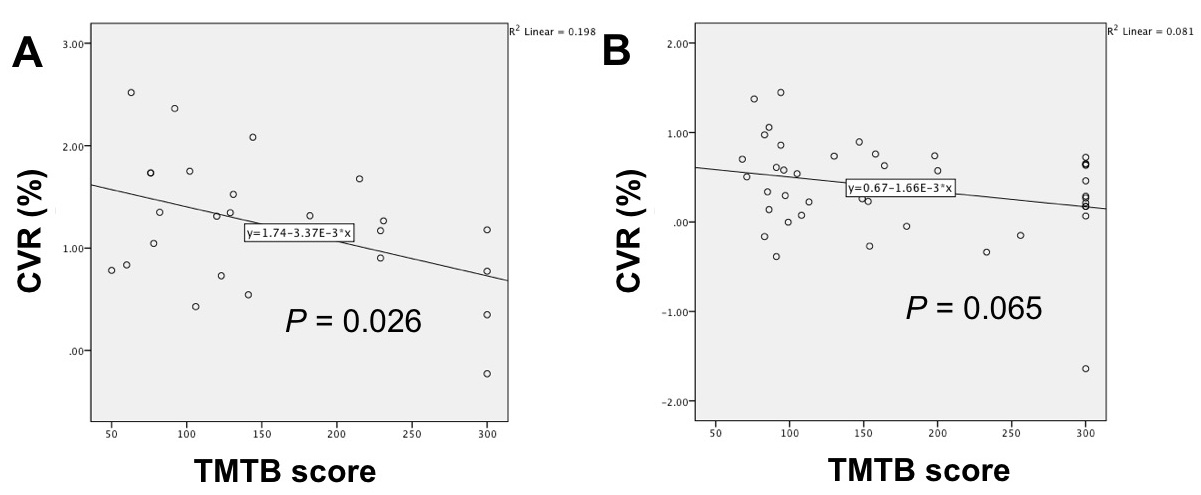
Fig 1 shows comparisons between the mean CVR values in AA and Caucasians. AA had lower CVR in white matter (WM) in the frontal lobe (0.353% ± 0.530%) than Caucasians (0.603% ± 0.454%) (P = 0.027), while no significant gender differences in CVR were observed. CVR values of grey matter (GM) (r = -0.289, P = 0.017) and WM (r = -0.288, P = 0.017) in the frontal lobe were associated with lower scores of TMTB (Fig 2), reflecting better performance on executive function. When stratified by race, Caucasians had a significant correlation in GM (r = -0.445, P = 0.026), while a trend toward significance in WM was observed among AA (r = -0.284, P = 0.065) (Fig 3).Discussion and Conclusion
Our findings provide evidence for correlation between decline in CVR and executive dysfunction among patients with MCI and hypertension, indicating the importance of CVR for cognitive function. Compared to Caucasians, hypertensive AA have more impaired cerebral microcirculatory function in both males and females. Our ongoing clinical trial will provide evidence if antihypertensive therapy will be associated with both executive function and CVR improvement, especially in AA.Acknowledgements
This research is supported by NIA/NIH grants RF1AG051633 and R01AG042127.References
1. Li, Y., et al., Cerebral angiography, blood flow and vascular reactivity in progressive hypertension. NeuroImage, 2015. 111: 329-337.
2. Silvestrini, M., et al., Cerebrovascular reactivity and cognitive decline in patients with Alzheimer disease. Stroke, 2006. 37(4): 1010.
3. Tang, M.-X., et al., Incidence of AD in African-Americans, Caribbean Hispanics, and Caucasians in northern Manhattan. Neurology, 2001. 56(1): 49-56.
Figures