2363
Motor cortex hypointensity on SWI is associated with APOE status in cognitive impaired patients1Radiology, Konkuk University Medical Center, SEOUL, Korea, Republic of, 2Neurology, Konkuk University Medical Center, SEOUL, Korea, Republic of
Synopsis
We evaluated the prevalence and its associated risk factors of motor cortex hypointensity on SWI in cognitive impaired patients. This retrospective study included 116 cognitively impaired patients (28 Alzheimer disease patients and 88 mild cognitive impaired patients). Among them, 83 patients showed positive motor cortex hypointensity on SWI and it was associated with age. Furthermore, the group with positive motor cortex hypointensity on SWI had less APOE4 allele carriers than negative group and this shows (+) APOE4 allele may act as an accelerating factor of cognitive decline even before iron accumulation starts to show changes in the motor cortex.
Purpose
Recently, motor cortex hypointensity on susceptibility-weighted imaging (SWI) has been introduced as an imaging marker of amyotrophic lateral sclerosis, which reflects in-vivo iron accumulation related to neuroinflammation and microgliosis. The hypointensity was also observed in normal elderly subjects.1-3 We hypothesized that motor cortex hypointensity, as a result of neurodegeneration associated with both aging and neuroinflammation, would be observed in cognitive impaired subjects. Hence, we aimed to evaluate motor cortex hypointensity on SWI in cognitive impaired subjects and to explore its associated risk factors.Methods
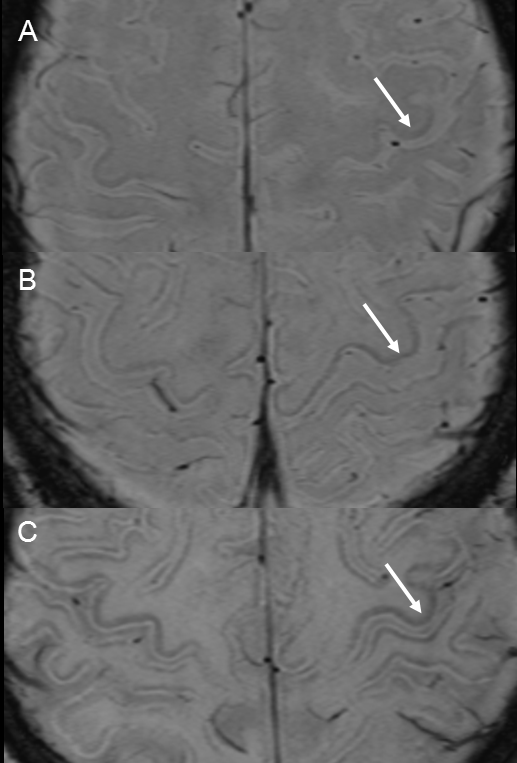
We analyzed SWIs of 116 cognitively impaired patients (28 with Alzheimer’s disease and 88 with mild cognitive impairments) who visited our memory clinic from Jan 2013 to Dec 2013. SWI was implemented using a 2D gradient-echo sequence, with TR=29ms, TE=20ms, flip-angle=15° and BW=120 Hz/pixel. Images were acquired with a 512×256 matrix, 22×22 cm2 FOV, and 72 slices at 2.0mm thickness, using the 3T MR scanner (Siemens Skyra) with a 20-channel phased array coil. Acquisition time was 3.13 min with a GRAPPA factor 2. All the SWI images were visually examined by two neuroradiologists at the any of bilateral precentral motor cortices compared to the postcentral sensory cortex; (A) (Score 0). (B) Mildly low signal intensity (Score 1). (C) Markedly low signal intensity (Score 2) (Fig 1). For statistical analysis, score of 1-2 was considered indicative of motor cortex hypointensity positive. Pearson χ2 test or Fisher’s exact test was applied to compare frequency of categorical variables and the Student t-test was used to compare continuous variables between positive motor cortical hypointensity. Interobserver agreement was evaluated using kappa statistics.Results
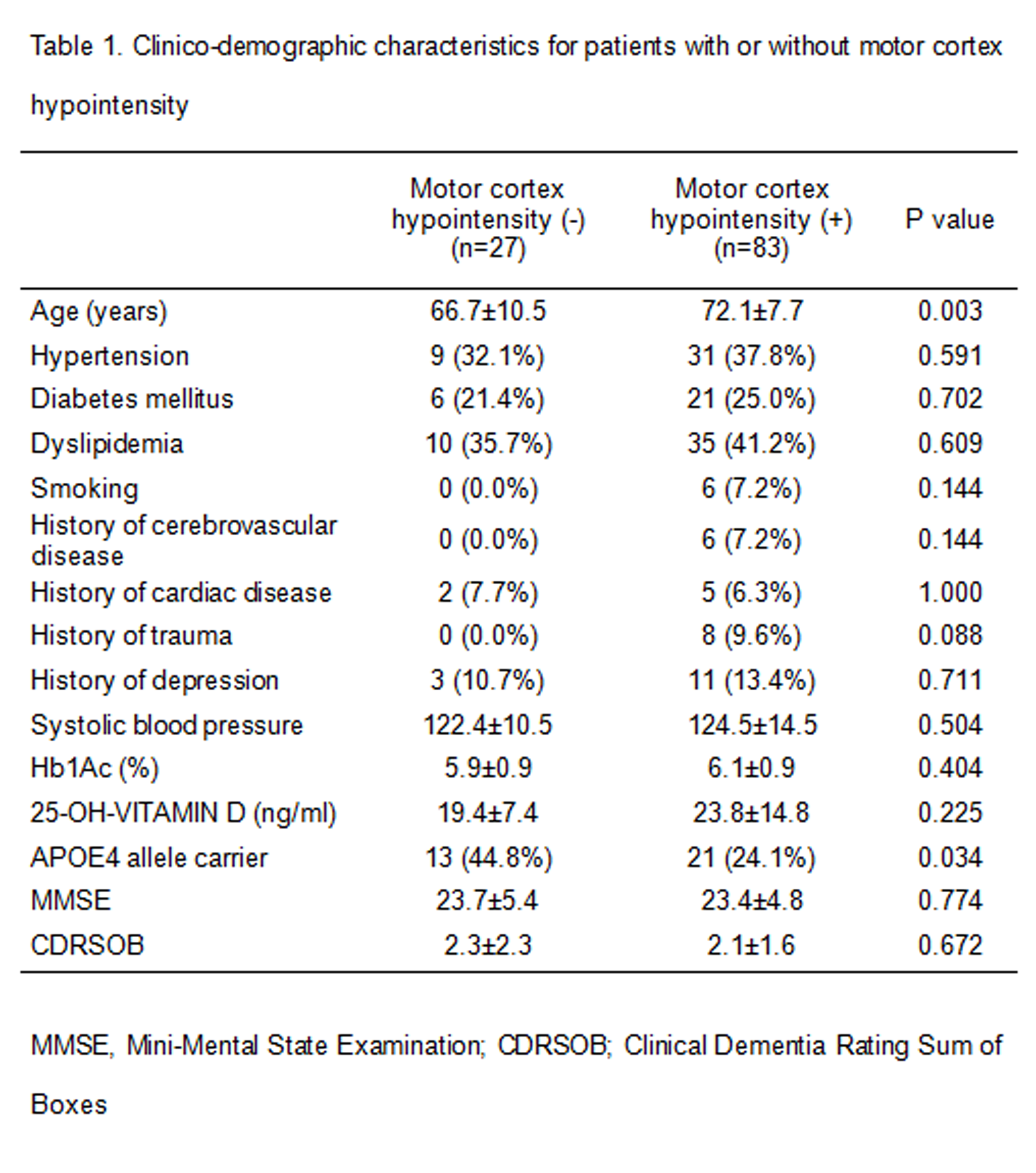
Among total 116 patients, we found 83 positive motor cortex hypointensity patients (71.6%). In positive motor cortex hypointensity group, (+) APOE4 allele carrier was less frequent than in negative group (24.1% vs 44.8%, P=0.034) but age was significantly higher in positive motor cortex hypointensity group than in negative group (72.1±7.7 years vs 66.7±10.5 years, P=0.003). There are no significant differences in clinical variables between positive and negative group including Mini-Mental State Examination and Clinical Dementia Rating Sum of Boxes (CDRSOB) scores (Table 1).Discussion and Conclusion
These data suggest positive motor cortex hypointensity is associated with (-) APOE4 allele status and age in cognitively impaired patients. As clinical severity was not different between positive and negative motor cortical hypointensity group, our findings suggest that (+) APOE4 allele status, the strongest genetic risk factor of Alzheimer disease,4 may accelerate cognitive decline even before iron accumulation starts to show changes in the motor cortex. Accordingly, iron accumulation and associated neurodegeneration may be more profound in the absence of APOE4 allele. Further studies are needed to determine the role of the motor cortex hypointensity as an imaging marker in cognitive impaired subjects.Acknowledgements
No acknowledgement found.References
1. Adachi Y, Sato N, Saito Y, et al. Usefulness of SWI for the Detection of Iron in the Motor Cortex in Amyotrophic Lateral Sclerosis. J Neuroimaging. 2015.25(3):443-451.
2. Costagli M, Donatelli G, Biagi L, et al. Magnetic susceptibility in the deep layers of the primary motor cortex in Amyotrophic Lateral Sclerosis. NeuroImage: Clinical. 2016.
3. Kamada K, Kakeda S, Ohnari N, Moriya J, Sato T, Korogi Y. Signal intensity of motor and sensory cortices on T2-weighted and FLAIR images: intraindividual comparison of 1.5T and 3T MRI. Eur Radiol. 2008.18(12):2949-2955.
4. Liu CC, Kanekiyo T, Xu H, Bu G. Apolipoprotein E and Alzheimer disease: risk, mechanisms and therapy. Nat Rev Neurol. 2013.9(2):106-118.
Figures