2323
Investigation of neuroinflammation and cognitive dysfunction following a major burn injury and critical care admission using advanced MR imaging1Department of Imaging, Imperial College Healthcare NHS Trust, London, United Kingdom, 2Department of Bioengineering, Imperial College London, London, United Kingdom, 3Department of Medicine, Imperial College London, London, United Kingdom, 4Magill Department of Anaesthesia, Chelsea and Westminster Hospital NHS Foundation Trust, London, United Kingdom, 5Department of Academic Anaesthesia, Imperial College London, London, United Kingdom, 6Department of Psychology, Westminster University, London, United Kingdom, 7Centre for Clinical Brain Sciences, University of Edinburgh, Edinburgh, United Kingdom
Synopsis
We used advanced MR imaging methods to investigate neurophysiological changes following major burns injury in a cohort of patients with reduced cognitive function compared to age and sex-matched controls. In this preliminary study, small regions of increased connectivity were observed in patients in two brain networks extracted from resting-state fMRI data using ICA. However, the significance of these results is unclear given the broad range of neurological functions implicated by the cognitive deficits. Furthermore, we found no significant difference between patients and controls for TBSS, volumetric analysis and MR spectroscopy. SWI indicated large areas of microbleeds in one patient.
Purpose
Survival of patients with major burns has improved significantly in the last few decades, but recent studies show that quality of life (QoL) is measurably reduced in burn survivors1. One year after injury about a fifth of patients meet the post-traumatic stress disorder diagnostic criteria2. It is hypothesised that this is caused by neuroinflammatory response following an excessive immune response to severe burns to peripheral tissue3. In this preliminary study we aim to investigate neurophysiological changes following major burns injury to the body and admission to intensive care using high resolution T1 weighted images, resting-state fMRI (rs-fMRI), diffusion tensor imaging (DTI), MR spectroscopy (MRS) and susceptibility weighted imaging (SWI), in a cohort of patients with a broad cognitive deficit.Methods
15 patients (11 male, 4 female; 25-74 years, mean 40.9 years) and 15 age and sex-matched controls were recruited to this prospective clinical study (1 patient-control pair was excluded from all but rs-fMRI analysis). Patients included were all admitted to the burn intensive care unit at Chelsea and Westminster Hospital between 2009 and 2015 with at least 15% total burn surface area (TBSA). Patients with toxic epidermal necrolysis syndrome, evidence of head trauma, and those for whom MRI was contraindicated were excluded. The study was approved by the research ethics committee and all participants gave informed consent. Cognitive and psychological testing showed patients had lower QoL and a broad cognitive deficit, which correlated with TBSA for certain tests. Participants underwent MRI, including T1 weighted imaging (1mm isotropic voxels), DTI (b=1000,30 directions, 2.5mm isotropic voxels), and single-voxel MRS (15 x 15 x 15 mm) in the posterior cingulate gyrus and the right frontal white matter. MELODIC in FSL software was used to decompose the rs-fMRI data into brain networks using independent component analysis (ICA) and connectivity in these networks patients and controls was compared using dual regression. FreeSurfer was used to extract brain regions from T1 images and compare the normalised volume of the hippocampus, amygdala and precuneus for patients and controls. DTI data were analysed using tract based spatial statistics (TBSS) in FSL and using FreeSurfer regions for the hippocampus, amygdala and precuneus. Cho/Cr, Cho/NAA and Ins/Cr ratios were extracted from MRS data using Tarquin. SWI images were reviewed for the presence of microbleeds by two neuroradiologists.Results
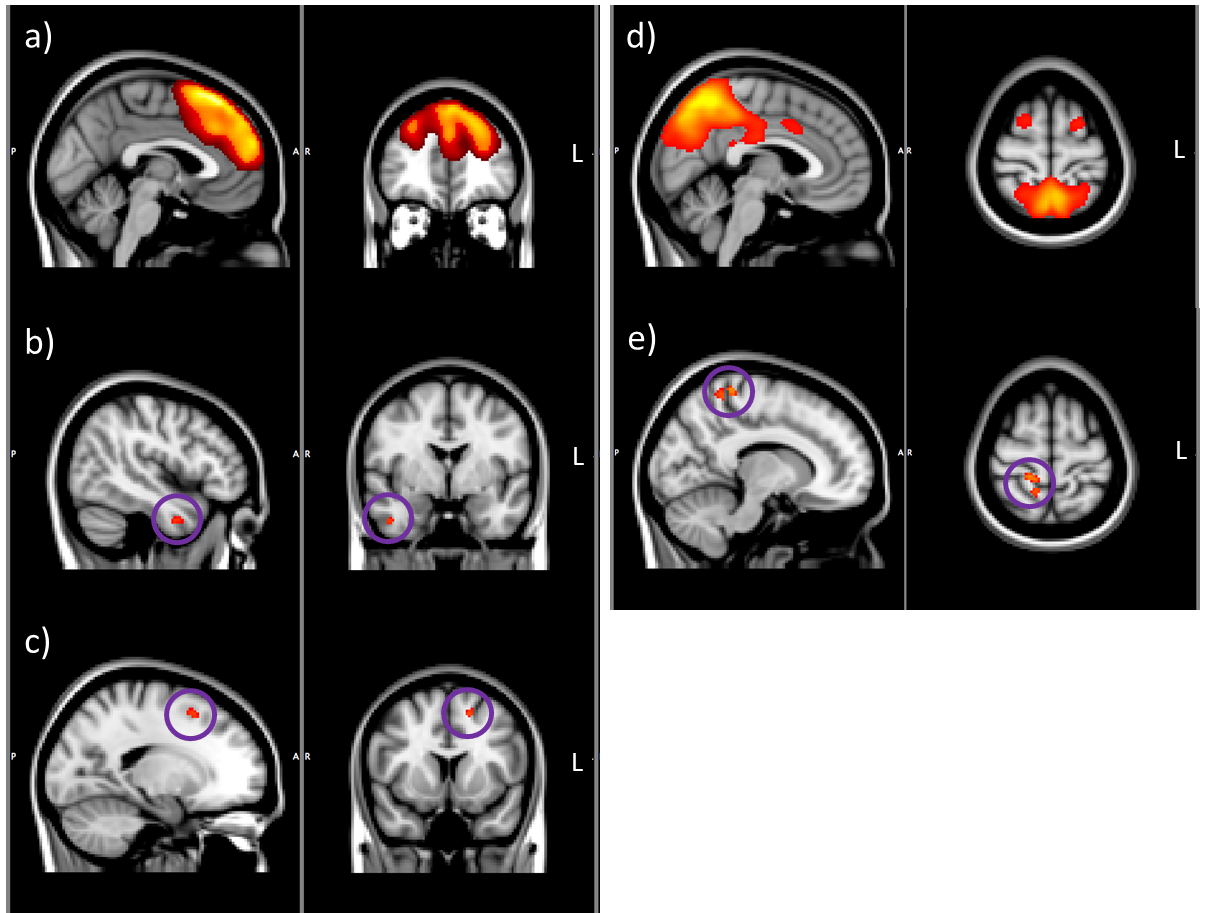
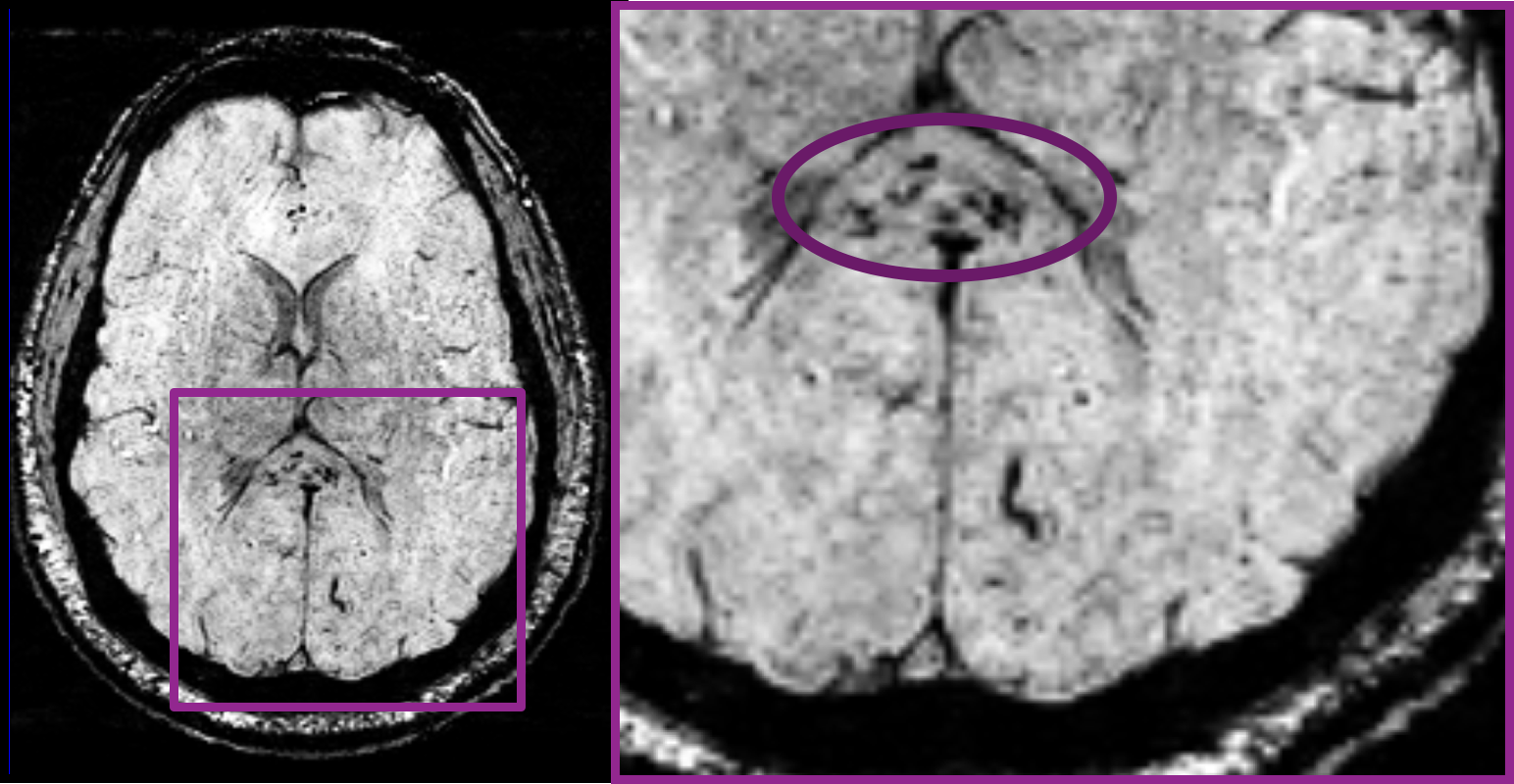
ICA of all 30 subjects resulted in 17 independent components. Dual regression showed no significant difference in patients compared to controls in 15 of the extracted brain networks, but small clusters of voxels showing a statistically significant increase in connectivity in two networks (Figure 1). When compared to the activation networks defined by Smith et al4 one of these ICAs most closely correlated to the “executive control” network and the other to the “default mode network” (cc=0.38 and 0.25 respectively). There were no significant differences for hippocampal and amygdala volumes between patients and controls. TBSS did not yield any statistically significant difference for differences between the two groups. There was also no significant difference for FA measurements in the hippocampus, amygdala and precuneus between patients and controls. Furthermore, no significant difference was observed between patients and controls for Cho/Cr, Cho/NAA and Ins/Cr ratios in both right frontal white matter and the posterior cingulate gyrus. A large number of microbleeds were identified in one patient in the corpus callosum (Figure 2). Two patients had one microbleed while no microbleeds were identified in 11 patients.Discussion
Severe burn injuries result in a systemic inflammatory response that can cause neuroinflammation; MRI during the acute and subacute phase has the potential to detect neuroinflammation non-invasively and provide prognostic biomarkers of future neurocognitive deficit and provide objective measures of the resultant long term damage. Cognitive testing in this cohort showed deficits covering a broad range of neurological functions. Therefore, it is difficult to identify a particular resting-state or white matter network to target for MR investigation and the pertinence of the small increase in connectivity observed in patients in the rs-fMRI data is unclear. Furthermore, no difference was observed between patients and controls in the other imaging methods used here. It is likely that the low patient numbers, wide range of TBSA (20 to 85 %, mean 38.4%) and particularly the large range in time since injury (9 months to 6.7 years, mean 3.5 years) may have confounded the results. Further study of imaging biomarkers in the early phases of burn injuries is warranted.Acknowledgements
MEF and MGS contributed equally to this work. MGS is funded by the Brain Tumour Charity and the Brain Tumour Research CampaignReferences
1. Goverman J, Mathews K, Nadler D, et al. Satisfaction with life after burn: A Burn Model System National Database Study. Burns. 2016;42(5):1067-73.
2. Esselman PC. Burn rehabilitation: an overview. Arch Phys Med Rehabil. 2007;88(12 Suppl 2):S3-6.
3. Flierl MA, Stahel PF, Touban BM, et al. Bench-to-bedside review: Burn-induced cerebral inflammation – a neglected entity? Critical Care. 2009;13(3):215.
4. Smith SM, Fox PT, Miller KL, et al. Correspondence of the brain’s functional architecture during activation and rest. PNAS. 2009;106(31):13040-5.
Figures