2309
Altered microstructural integrity of white matter tracts in children with aromatic L-amino acid decarboxylase deficiency1Institute of Medical Device and Imaging, National Taiwan University College of Medicine, Taipei, Taiwan, 2Institute of Biomedical Engineering, National Taiwan University College of Medicine, Taipei, Taiwan, 3Department of Medical Genetics, National Taiwan University Hospital and National Taiwan University College of Medicine, Taipei, Taiwan, 4Department of Pediatrics, National Taiwan University Hospital and National Taiwan University College of Medicine, Taipei, Taiwan, 5Graduate Institute of Brain and Mind Sciences, National Taiwan University College of Medicine, Taipei, Taiwan, 6Molecular Imaging Center, National Taiwan University, Taipei, Taiwan
Synopsis
Aromatic L-amino acid decarboxylase (AADC) deficiency is an inherited disorder that impairs synthesis of dopamine and serotonin. To investigate whether the white matter tracts are impaired in children with AADC deficiency, diffusion tensor imaging data were obtained from 7 children with AADC deficiency and 7 matched controls. Fractional anisotropy (FA) of 76 white matter tracts was measured and compared between the two groups. Fiber tracts of dopaminergic and serotonergic systems, and those connecting regions responsible for executive functions or regulating motor functions showed lower FA in patients. Our findings are consistent with clinical manifestations and pathophysiology of AADC deficiency.
Purpose
Aromatic L-amino acid decarboxylase (AADC) deficiency is a rare inherited disorder that impairs synthesis of dopamine and serotonin. Children with AADC deficiency exhibit severe motor, behavioral, and autonomic dysfunctions. We hypothesized white matter integrity of the tracts relevant to these functions should be altered in children with AADC deficiency. Therefore, a tract-specific analysis of the whole brain was performed on diffusion tensor imaging (DTI) data to investigate the patterns of tract alteration in AADC.Methods
The subjects consisted of 7 children with clinical diagnosis of AADC deficiency (gender: 3 males and 4 females, age: 4.86±2.48 years) and 7 age- and sex-matched healthy control children. MR scanning was performed on a 1.5T MRI system (Signa HDx, GE). DTI was acquired using an echo planar imaging (EPI) sequence, TR/TE = 7000/105 ms, FOV = 110 × 110 mm, image matrix size 128 × 128, and 5 mm slice thick. A total of 42 diffusion encoding gradients with the maximum diffusion sensitivity bmax = 1000 s/mm^2 were applied to acquire diffusion datasets. T1-weighted imaging was performed using a 3D fast spoiled gradient echo (FSPGR) sequence: repetition time (TR) / echo time (TE) = 10 ms/4 ms, flip angle = 12°, FOV = 94 × 94 mm^2, acquisition matrix = 192 × 192, and 1 mm slice thick. Whole brain tract-specific analysis was performed using tract-based automatic analysis1 (TBAA). The procedure of TBAA entailed the following. 1) Study subjects were registered to create a study specific template (SST) using large deformation diffeomorphic metric mapping2. 2) The SST was registered to a diffusion template in the standard space3. 3) Sampling coordinates of 76 tracts were transformed from the diffusion template to individual DTI datasets via the transformation matrix between the template and SST as well as the transformation between the SST and individual DTI. 4) Fractional anisotropy (FA) values were sampled in the native DTI space using the transformed sampling coordinates and a 2D array of FA profiles along 76 tracts, named connectogram, was created for each subject. Two sample T-test was performed to investigate the difference of mean FA values between the two groups. A threshold free cluster weighted (TFCW) method was used following Smith’s approach4 to estimate weighted scores $$$S(p)=\sum_{h=h_0}^{h_5} e_{p}(h)$$$, where ep was the cluster extent level at step p which survived at a given threshold h of the effect size. A 98% cut-point of the histogram of TFCW scores was estimated to determine the most different clusters of FA in tracts between the two study groups.
Results
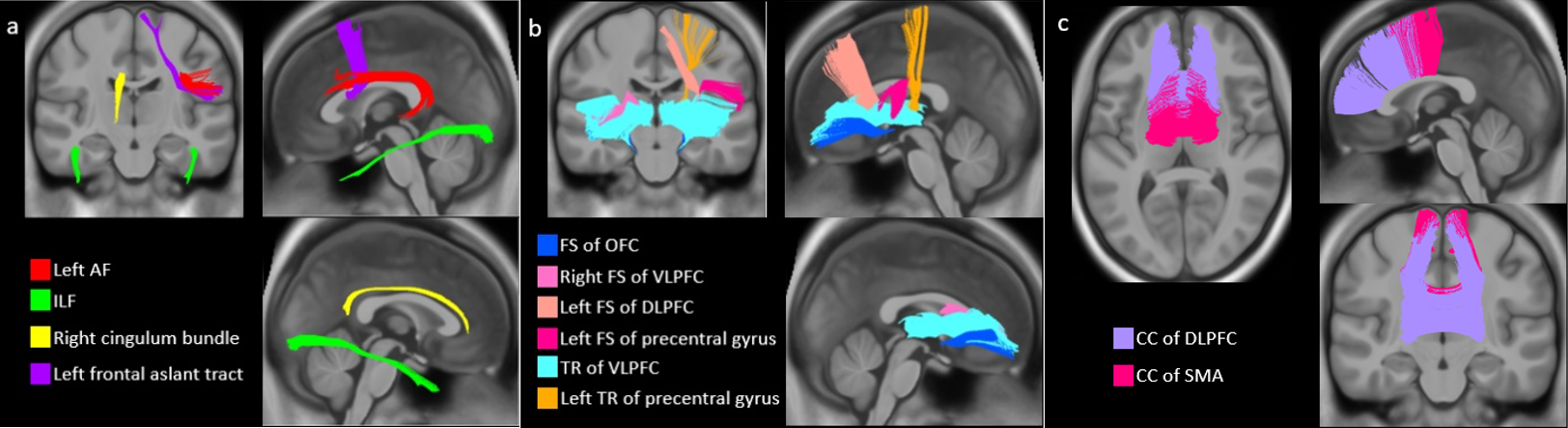
Mean FA was reduced in the bilateral fibers of frontostriatal (FS) circuits of the orbitofrontal cortex (OFC), and the callosal fibers (CF) of the dorsal lateral prefrontal cortex (DLPFC) (p < 0.05, uncorrected). The TFCW estimation revealed 15 tract segments that were in the top 2 percentile of the histogram; they were located in the left arcuate fasciculus (AF), right cingulum bundle (main body part), left frontal aslant tract, bilateral inferior longitudinal fasciculus (ILF), right FS of the ventral lateral prefrontal cortex (VLPFC), left FS of the DLPFC, left FS of the precentral gyrus, bilateral thalamic radiation (TR) of the VLPFC, left TR of the precentral gyrus, and CF of the supplementary motor area (SMA). These tracts were visualized in three fiber systems, namely association (Figure 1a), projection (Figure 1b) and commissure fiber systems (Figure 1c).Discussion
This is the first study to systematically investigate the microstructural alterations of white matter tracts in AADC deficiency. The FS circuit, which forms the connections between the striatum and frontal cortex, is dominated by dopaminergic and serotonergic systems. Since AADC deficiency leads to reduced production of dopamine and serotonin, which might explain the decreased FA in FS connections. We also found lower FA in tracts that are related to regions responsible for executive functions (DLPFC and OFC) and regions regulating motor functions (VLPFC and precentral gyrus). This might explain the developmental delay and motor dysfunction in AADC deficiency. In conclusion, children with AADC deficiency show altered microstructural integrity of the white matter tracts that are consistent with clinical manifestations and pathophysiology of the disease.Perspective
Dr. Hwu and his colleagues have been developing novel gene therapy for AADC deficiency5. Preliminary results of patients with one-year gene therapy indicated that there might be a recovery process in white matter integrity due to therapy. A longitudinal neuroimaging study with a sufficient sample size is warranted to clarify the effects of therapy on the microstructure of the white matter tracts.Acknowledgements
No acknowledgement found.References
1. Chen, Y., Lo, Y., Hsu, Y., Fan, C., Hwang, T., Liu, C., Chien, Y., Hsieh, M., Liu, C., Hwu, H. and Tseng, W. (2015). Automatic whole brain tract-based analysis using predefined tracts in a diffusion spectrum imaging template and an accurate registration strategy. Human Brain Mapping, 36(9), pp.3441-3458.
2. Hsu, Y., Hsu, C. and Tseng, W. (2012).A large deformation diffeomorphic metric mapping solution for diffusion spectrum imaging datasets. NeuroImage, 63(2), pp.818-834.
3. Hsu, Y., Lo, Y., Chen, Y., Wedeen, V. and Isaac Tseng, W. (2015). NTU-DSI-122: A diffusion spectrum imaging template with high anatomical matching to the ICBM-152 space. Human Brain Mapping, 36(9), pp.3528-3541.
4. SMITH, S. and NICHOLS, T. (2009). Threshold-free cluster enhancement: Addressing problems of smoothing, threshold dependence and localisation in cluster inference. NeuroImage, 44(1), pp.83-98.
5. Lee, N., Muramatsu, S., Chien, Y., Liu, W., Wang, W., Cheng, C., Hu, M., Chen, P., Tzen, K., Byrne, B. and Hwu, W. (2015). Benefits of Neuronal Preferential Systemic Gene Therapy for Neurotransmitter Deficiency. Mol Ther, 23(10), pp.1572-1581.
Figures