2298
Multi-shell Multi-band Diffusion Imaging (MSMBDI) is more predictive of executive deficits in Preadolescents with Complex Congenital Heart Disease (CHD) compared to standard diffusion tensor imaging (DTI)1Radiology, University of Pittsburgh, Pittsburgh, PA, United States, 2Radiology, Children's Hospital of Pittsburgh UPMC, Pittsburgh, PA, United States, 3Psychology, Carnegie Mellon University, Pittsburgh, PA, United States, 4Neurological Surgery, University of Pittsburgh, Pittsburgh, PA, United States, 5Developmental Biology, University of Pittsburgh, Pittsburgh, PA, United States
Synopsis
We tested whether Multi-shell Multi-band Diffusion Imaging (MSMBDI) would be superior to standard DTI at delineating microstructural cortical association fiber abnormalities and predicting executive function preadolescents with complex congenital heart disease (CHD). Using both a hypothesis-driven approach (manual tractography) and a data-driven approach (q-space diffeomorphic reconstruction) we examined white matter tracts in correlation with NIH Toolbox and complementary battery of neuropsychological test. We show that MSMBDI – when compared to standard DTI – showed greater sensitivity towards white matter structure differences, superior at detecting microstructural differences in cortical association tracts in CHD compared to controls, and more predictive of executive deficits.
Introduction
Preadolescent subjects with complex congenital heart disease (CHD) demonstrate deficits in executive function related to microstructural vulnerability of cortical association fibers (Reference). Multi-shell Multi-band Diffusion Imaging (MSMBDI) provides improved delineation of crossing fibers within periventricular white matter. We tested the hypothesis that MSMBDI would be superior to standard diffusion tensor imaging (DTI) with regard to not only delineating microstructural cortical association fiber abnormalities but also predicting executive function deficits in preadolescents with CHD.Materials and Methods
A total of 84 pediatric/adolescent subjects (CHD = 44, 13.4±3.6 y.o.; controls=40, 13.5±3.9 y.o.) were prospectively recruited, with 74 completing MRI scans and NIH Tool Box neurocognitive assessment. Participants were scanned on a Siemens 3T Skyra system using a 32-channel head coil – each receiving a DTI and a MSMBDI. The DTI sequence had the following parameters: FOV = 256mm, voxel size = 2.0mm (isotropic), TE/TR=92ms/12600ms, and 42-directions at B=1000s/ mm2. The echo-planar MBMSDI: FOV=240mm, voxel size=2.4mm (isotropic), matrix size=100x100x60, multiband-factor=3, and 128-directions each at B=3000s/mm2 (at TE/TR=110ms/3300ms) and B=5000s/ mm2 (at TE/TR=130ms/3600ms).
The DTI and MSMBDI images were processed in DSI studio (Organization, Place) with DTI and GQI reconstructions, respectively, using both a hypothesis-driven approach (manual tractography) and a data-driven approach - q-space difeomorphic reconstruction (QSDR)1. A standardized uniform placement of ROIs and Region of Avoidance (ROAs) were used to generate corticospinal tracts (CST), genu and splenium of the corpus callosum, and superior longitudinal fasciculi (SLF). Average fractional anisotropy (FA) for DTI and normalized quantitative anisotropy (nQA) for MSMBDI were computed over each tract. The same images were then reconstructed and registered into common space using the QSDR technique in DSI studio for the voxel-based analysis2,3.
Cognitive assessment was conducted using NIH Toolbox (NIHTB)4 and a battery of neuropsychological tests including the Wechsler Abbreviated Scale of Intelligence II (WASI-II), Delis–Kaplan Executive Function System (D-KEFS), and the Behavior Rating Inventory of Executive Functioning (BRIEF), with emphasis on executive function.
An initial analysis to examine differences between CHD and Controls was conducted using Student’s T-Tests on average FA and nQA, and normalized age-corrected assessment scores for the respective neuropsychological tests. This was followed by a linear regression correlating neurocognitive scores with imaging metrics (average FA and nQA) of the generated tracts with CHD status as a covariate.
Results
Using the hypothesis-driven approach (manual tractography), both DTI and MSMBDI demonstrated reduced FA(p=0.026) and nQA (p=0.046) for the splenium, in CHD compared to healthy controls. However, MSMBDI showed additional reductions in the genu (p=0.016) and SLF (p=0.034 left, p=0.013 right) in CHD compared to controls.
The T-Test on cognitive tests showed CHDs tended to score worse than controls in NIHTB Oral Reading Recognition (p=0.005) and D-KEFS Trail Making-Number Sequencing tests (p=0.034).
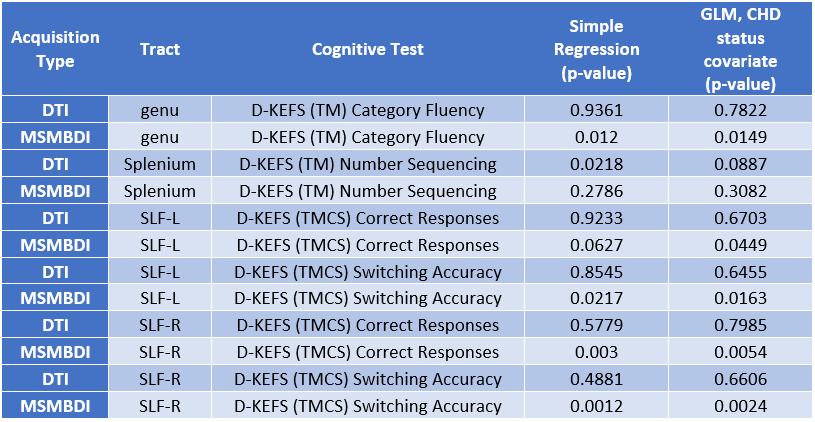
For MSMBDI, there was a significant correlation between nQA in the SLF and DKEFS Trail Making-Category Switching (TMCS): Correct Responses, Switching Accuracy; and nQA in the genu and D-KEFS (TM) Category Fluency. These associations still held when modeled with CHD status as a covariate. (Table 1). In contrast, most of the DTI derived tracks did not show any correlation, except for FA in the splenium and D-KEFS Trail Making (TM) Number Sequencing.
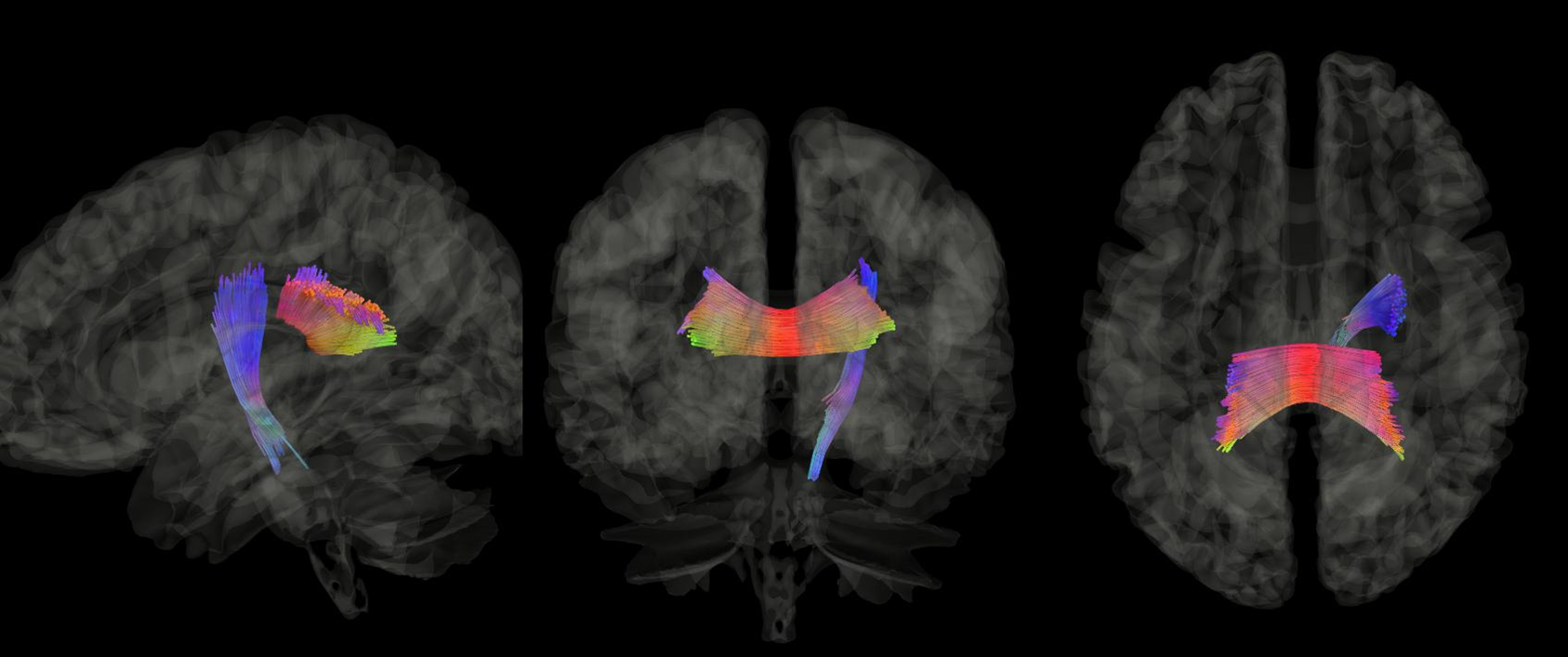
Interestingly, using the data-driven approach (QSDR- voxel based), standard DTI delineated reduced connectivity in the splenium and segment of right CST in the CHD cases compared to controls (Figure 1) (as measured by spin density function) (p=0.04, FDR corrected). The QSDR voxel-based analysis using only MSMBDI showed no statistically significant regions of difference between CHDs and controls.
Discussion
Using a hypothesis-driven manual tractography approach, we show that MSMBDI is superior to conventional DTI at detecting microstructural differences in cortical association tracts in pre-adolescent CHD compared to healthy controls. The MSMBDI derived tracts (nQA) showed greater sensitivity towards white matter structure differences in the genu and SLF. In addition, MSMBDI generated tracks were more predictive of executive deficits when compared to standard DTI. The data-driven voxel-based QSDR technique was able to show differences at the voxel level using standard DTI, but failed to detect these differences with MSMBDI. The high b-value (5000s/mm2), optimized for end-to-end connectometry, may lead to the negation of subtle differences at the voxel level.Conclusion
Using manual tractography, MSMBDI is superior to conventional DTI in detecting alterations in cortical association microstructure and associated executive deficits in preadolescent CHD compared to controls.Acknowledgements
Michelle Gruss (Department of Radiology, Children's Hospital), Cheryl Burns (University of Pittsburgh Medical Center)
References
[1] Yeh, F.C., Wedeen, V.J. and Tseng, W.Y.I., 2010. Generalized-sampling imaging. IEEE transactions on medical imaging, 29(9), pp.1626-1635.
[2] Yeh, F.C. and Tseng, W.Y.I., 2011. NTU-90: a high angular resolution brain atlas constructed by q-space diffeomorphic reconstruction. Neuroimage,58(1), pp.91-99.
[3] Yeh, F.C., Verstynen, T.D., Wang, Y., Fernández-Miranda, J.C. and Tseng, W.Y.I., 2013. Deterministic diffusion fiber tracking improved by quantitative anisotropy. PloS one, 8(11), p.e80713.
[4] Gershon, R.C., Cella, D., Fox, N.A., Havlik, R.J., Hendrie, H.C. and Wagster, M.V., 2010. Assessment of neurological and behavioural function: the NIH Toolbox. The Lancet Neurology, 9(2), pp.138-139.
Figures