2252
Pretreatment PET and MRI imaging markers of lithium treatment response/nonresponse in patients with bipolar depression1Psychiatry, Stony Brook Medicine, Stony Brook, NY, United States, 2Radiology, Stony Brook Medicine, Stony Brook, NY, United States, 3Biomedical Engineering, Stony Brook University, Stony Brook, NY, United States, 4Neurobiology & Behavior, Stony Brook University, Stony Brook, NY, United States
Synopsis
Bipolar disorder is one of the most prevalent psychiatric diseases in developed countries, and virtually all major psychiatric associations recommend lithium as the first line therapy for bipolar patients in the depressive phase of the illness, despite relatively low response rate for the drug and relatively high likelihood of side effects. However, no predictive criteria which indicate an individual patient’s responsiveness to lithium are employed clinically. In this work, we present preliminary findings demonstrating an association between baseline, multimodal neuroimaging measurements and lithium treatment outcome.
Purpose
Bipolar disorder (BD) is one of the most prevalent psychiatric diseases in developed countries, with an estimated lifetime prevalence of 1.3%1. The World Health Organization considers BD the sixth largest public health burden among mental disorders as determined by disability adjusted life years2.
Virtually all major psychiatric associations recommend lithium as the first line therapy for BD patients in the depressive phase of the illness (bipolar depression, BPD)3, despite relatively low response rate for the drug4,5 and relatively high likelihood of side effects6-10. Whereas lithium therapy exhibits several non-idealities, no predictive criteria which indicate an individual patient’s responsiveness to lithium are employed clinically. In this work, we present preliminary findings demonstrating an association between baseline, multimodal neuroimaging measurements and lithium treatment outcome.
Methods
We scanned 13 BD patients on separate PET and MR scanners before they began 6-8 weeks of lithium monotherapy. Serotonin 1A autoreceptor (5HT1A) binding potential was measured using dynamic [11C]-CUMI-101 PET with metabolite-corrected arterial input function; MRI acquisition was performed on 3T Siemens scanners (Trio or Skyra) included structural (MPRAGE, TR/TE/TI=2300/2.98/900ms, FA=9°, 1x1x1mm3 resolution) , resting state fMRI (TR/TE=2310/28ms, 3.2x3.2x3.2mm3 resolution, 2 sessions, 7 minutes each), arterial spin labeling (ASL, 2D multi-slice pCASL: TR/TE=4460/17 ms, 3.5x3.5x5mm3 resolution with 30 slices, labeling time 1.6s, post-labeling delay 1.5s) and diffusion tensor imaging (DTI, TR/TE=8300/95ms, 64 directions, b=1000, 2.5x2.5x2.5mm3 resolution). Patients were assessed using the 17-item Hamilton Depression Rating Scale (HDRS) both prior to and 6-8 weeks after their treatment with lithium. Baseline imaging measurements were correlated to reduction in symptom severity as reflected by HDRS using linear regression. Regions of interest (dorsal raphe nuclei [raphe, only used for PET analysis], amygdala, temporal pole, prefrontal cortex [PFC]) were preselected based on existing literature. Linear regression was used to assess the relationship between neuroimaging measurements and treatment outcome. Data analysis focused on preselected regions of interest based on the literature. Spearman's rank correlation analysis was performed in Matlab; correlation coefficient and p values are reported as rrank and Prank.Results
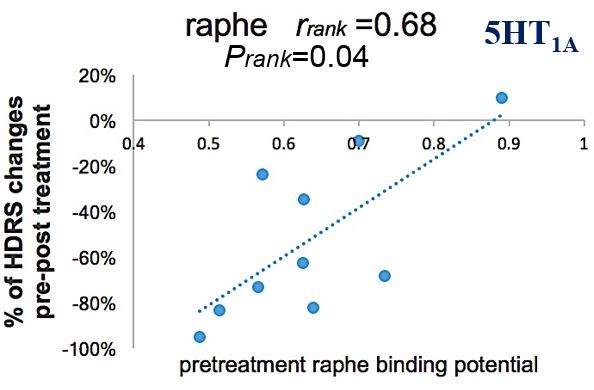
[11C]-CUMI-101 data were available for 10 patients. A statistically significant correlation between raphe 5HT1A binding potential and symptom reduction was observed (Figure 1), with lower baseline binding potential (BPND) in the raphe indicating better treatment outcome.
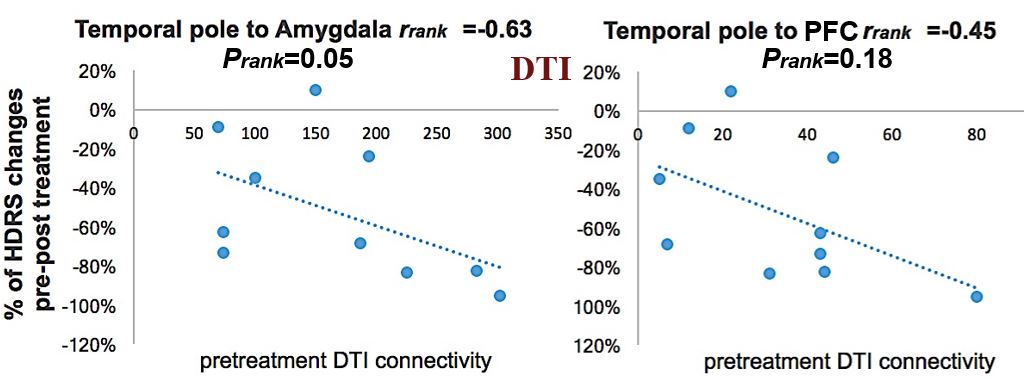
DTI data were available for 10 patients. Baseline connectivity (measured by number of streamlines connecting two regions reconstructed using DSI-studio with whole-brain seeding) between the temporal pole and amygdala was significantly correlated to symptom reduction, with a correlation between temporal pole to prefrontal cortex connectivity existing at trend level (Figure 2).
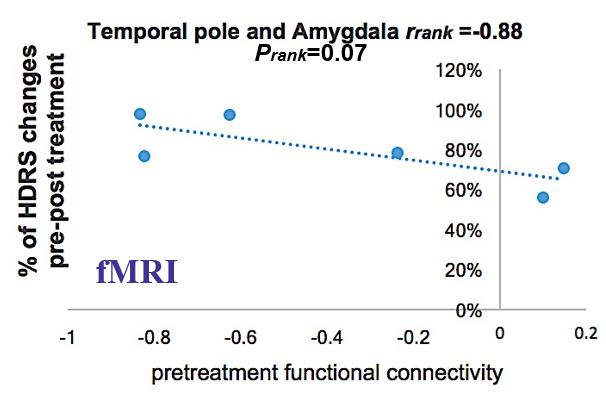
Six patients were scanned using resting state fMRI. Patients with higher baseline functional connectivity between the temporal pole and amygdala had generally better treatment outcomes (Figure 3).
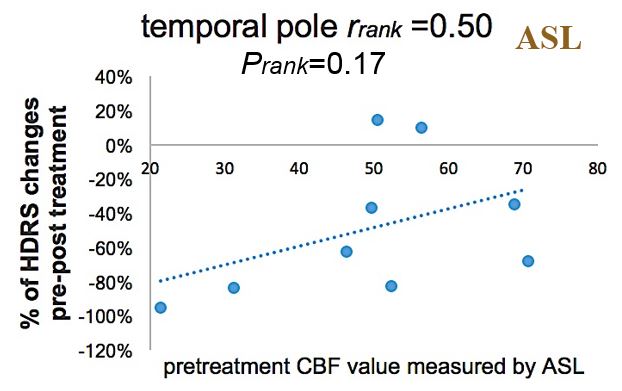
Arterial Spin Labeling (ASL) data were available in 9 of the 13 patients. ASLtbx package with partial volume correction was utilized for perfusion quantification11. A correlation between pretreatment blood flow to the temporal pole existed at trend level (Figure 4), with lower blood flow in the region associated with greater reduction in symptoms
Discussion
We observed modest correlation between responsiveness to lithium treatment and several neuroimaging markers probing different aspects of neurobiology in a small cohort of patients experiencing BPD. To the best of our knowledge this represents the first dedicated effort to examine lithium treatment prediction in such a population using multi-modal imaging.
Whereas several correlations existed only at trend level, this may be a reflection of our modest sample size. Regardless of the significance of any single predictive criterion, documenting such trends could allow for the creation of a combined model for treatment outcome, utilizing data from several neuroimaging markers to give a direct prognostic outcome for an individual patient. Unfortunately, the lack of complete datasets for each patient obviates the possibility of examining such a model in the current work.
A larger study utilizing these techniques to examine lithium treatment prediction could profoundly improve the standard of care for BPD patients. Medication adherence in this population is notably low, leading to reduced treatment efficacy and increased economic costs. The future ability to determine individualized prognostic scores for lithium treatment would not only help physicians more rapidly ameliorate symptoms by prescribing alternative medication to likely nonresponders, but also encourage those who should respond well to lithium to adhere to their treatments.
Conclusion
The preliminary data presented here demonstrate the potential of multimodal neuroimaging in predicting treatment response. Future prospective work in a larger patient population, particularly one with sufficient size to control for treatment moderating effects of biological variables such as sex and age, is warranted.Acknowledgements
NIH R01MH090276References
1. Kleinman, L.S., et al., Costs of bipolar disorder. Pharmacoeconomics, 2003. 21(9): p. 601-622.
2. Whiteford, H.A., et al., Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. The Lancet, 2013. 382(9904): p. 1575-1586.
3. Fountoulakis, K., et al., Treatment guidelines for bipolar disorder: a critical review. Journal of affective disorders, 2005. 86(1): p. 1-10.
4. Manchia, M., et al., Assessment of response to lithium maintenance treatment in bipolar disorder: a Consortium on Lithium Genetics (ConLiGen) report. PLoS One, 2013. 8(6): p. e65636.
5. Rybakowski, J.K., Response to lithium in bipolar disorder: clinical and genetic findings. ACS chemical neuroscience, 2014. 5(6): p. 413-421.
6. Close, H., et al., Renal failure in lithium-treated bipolar disorder: a retrospective cohort study. PLoS One, 2014. 9(3): p. e90169.
7. Monteith, S., et al., Big data for bipolar disorder. International journal of bipolar disorders, 2016. 4(1): p. 1.
8. Suppes, T., et al., Risk of recurrence following discontinuation of lithium treatment in bipolar disorder. Archives of General Psychiatry, 1991. 48(12): p. 1082-1088.
9. Dols, A., et al., The prevalence and management of side effects of lithium and anticonvulsants as mood stabilizers in bipolar disorder from a clinical perspective: a review. International clinical psychopharmacology, 2013. 28(6): p. 287-296.
10. Honeycutt, A.A., et al., Medical costs of CKD in the Medicare population. Journal of the American Society of Nephrology, 2013. 24(9): p. 1478-1483.
11. Liang, X., A. Connelly, and F. Calamante, Improved partial volume correction for single inversion time arterial spin labeling data. Magn Reson Med, 2013. 69(2): p. 531-7.
Figures