2164
2D-Turbo Spin-Echo Sequence with Incremental Trigger Delay Time for Monitoring Vascular Signal Suppression in Peripheral Pulse Gated Black-blood Lung MR Imaging1Department of Clinical Radiology, Kyushu University Graduate School of Medical Sciences, Fukuoka, Japan, 2Department of Molecular Imaging and Diagnosis, Kyushu University Graduate School of Medical Sciences, Fukuoka, Japan, 3Philips Electronics Japan, Ltd, Tokyo, Japan
Synopsis
Breath-hold black-blood magnetic resonance imaging of the lung provides promising results in focal lesion detection. Using peripheral pulse gating, we intended to monitor the degree of vascular suppression and the changes in tissue contrast more closely than in the previously reported methods. Black-blood fat-saturated T2-weighted images were acquired for healthy volunteers with incremental delay time points throughout the pulse cycle. The relative ratios of the specific tissue to the muscle were quantified. The systolic phase provided superior black-blood effects and was considered optimal for signal acquisition.
Purpose
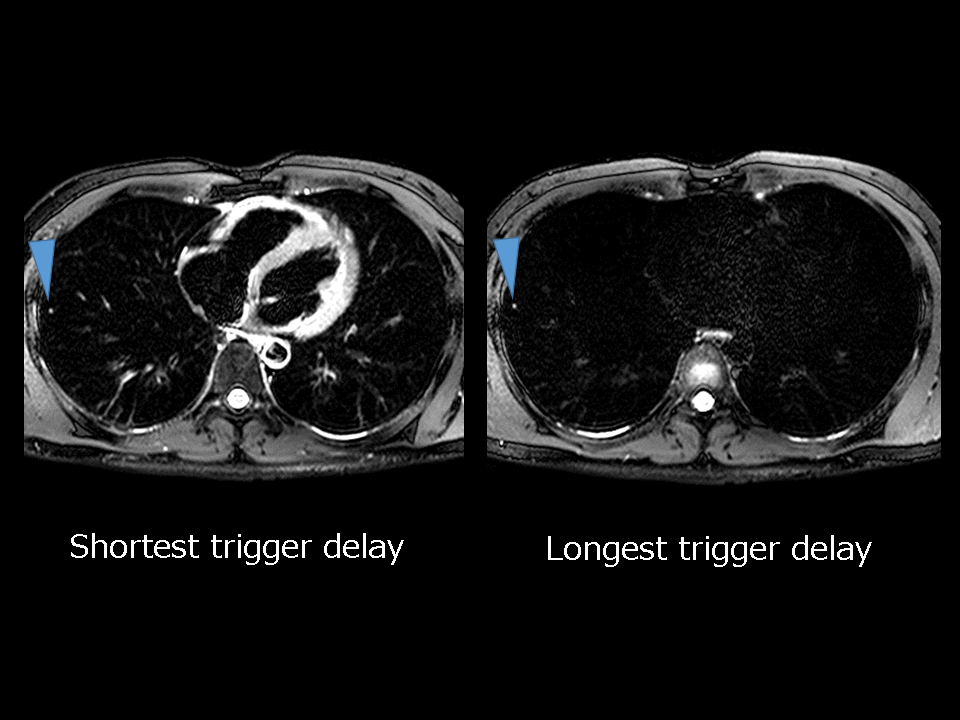
Single-shot turbo spin-echo (SSTSE) T2-weighted imaging (T2WI) is frequently used for rapid lung MR imaging. However, on SSTSE-T2WI, flow-related artifacts arising from major vessels can obscure small or subsolid lesions. The black-blood technique can suppress the intravascular signal and can improve lesion conspicuity. We previously demonstrated that breath-hold black-blood fat-saturated T2WI (BB-FST2WI) enables the precise detection and size measurement of both solid nodules and focal ground-glass opacities1. However, incomplete signal suppression was occasionally observed, which led to false-positive findings. Our preliminary results showed that BB-FST2WI in combination with peripheral pulse unit (PPU) gating allows effective signal suppression with data sampling in the longest trigger delay time2 (Figure 1). Thus, it should be necessary to monitor the vascular signal suppression during a cardiac cycle in order to obtain BB-FST2WI with vascular signal fully suppressed. The aim of this study was to evaluate the feasibility of 2D-TSE sequence with incremental trigger delay time for continuous monitoring of the vascular signal suppression in black-blood lung MR imaging and to determine the optimal delay time with respect to signal suppression of pulmonary vessels and tissue contrast.Materials and Methods
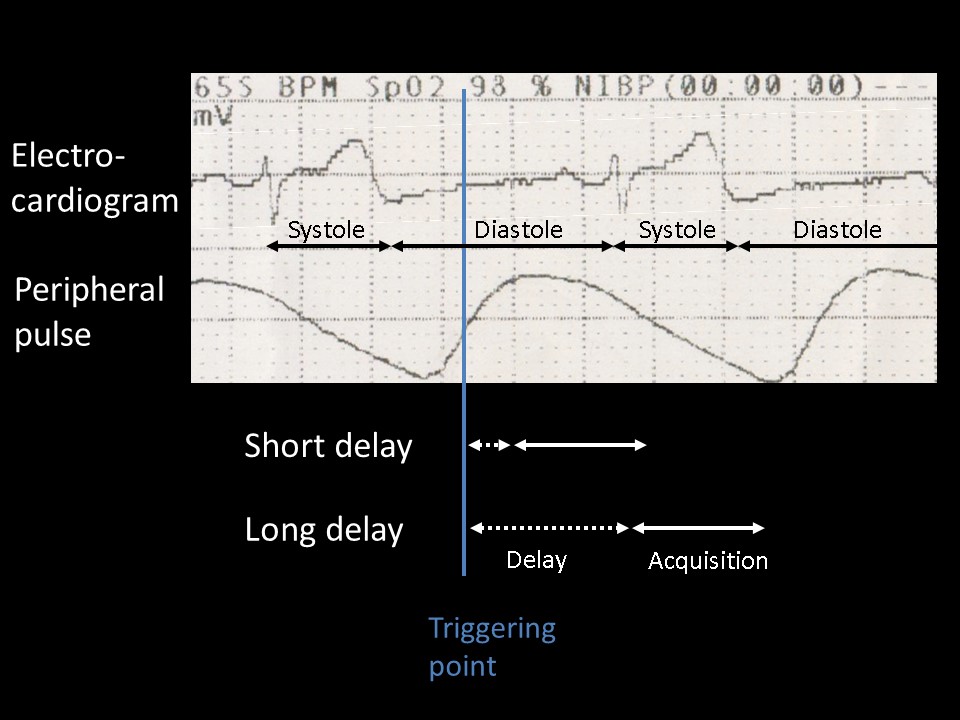
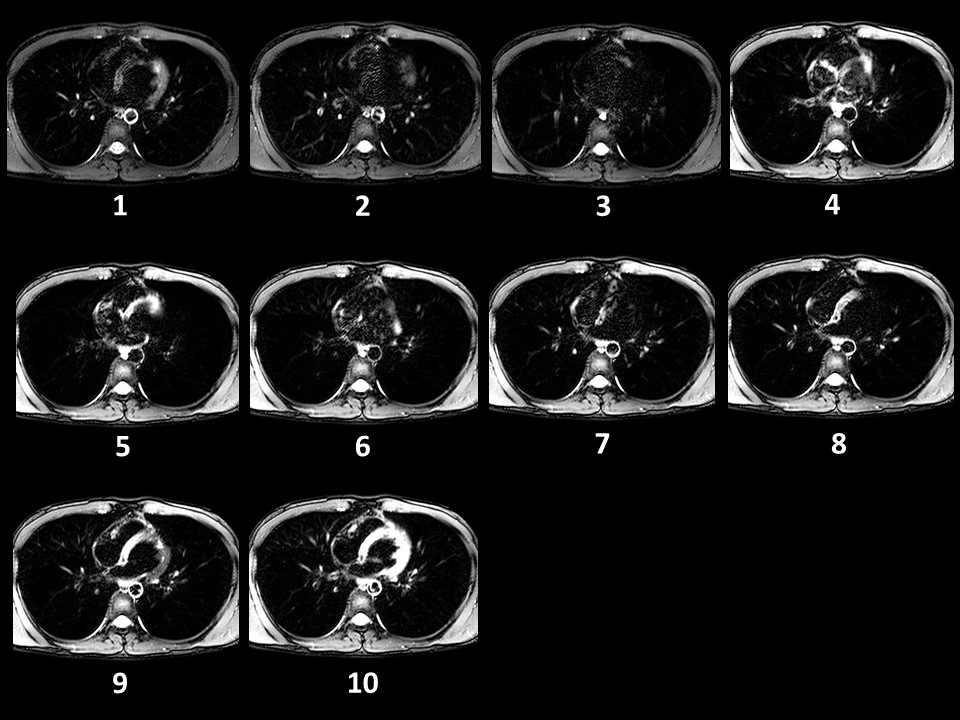
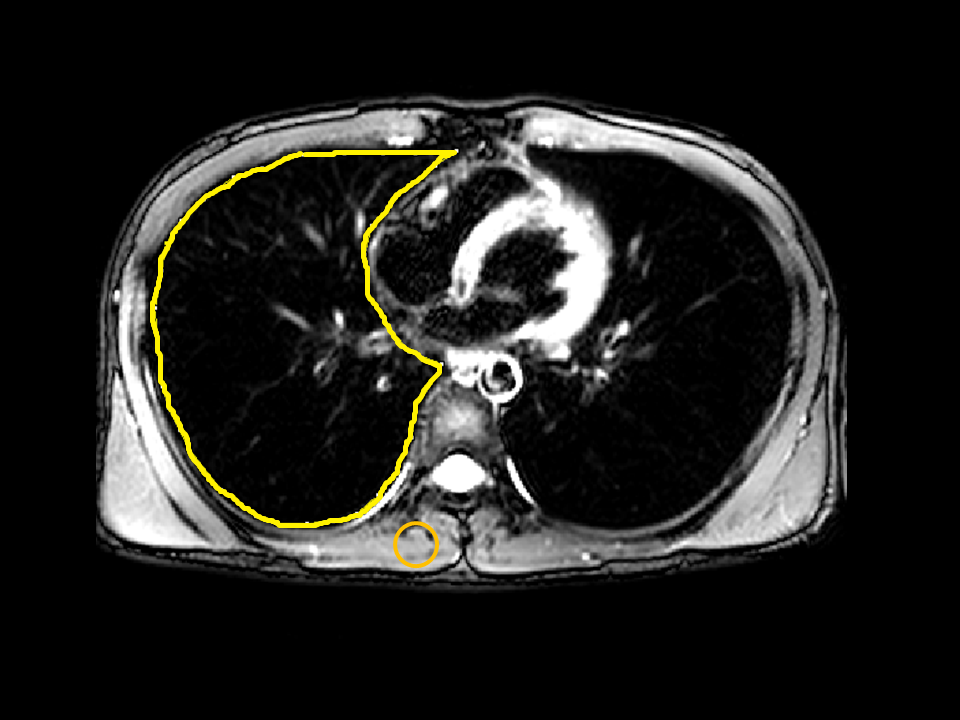
Eight healthy male volunteers (age, 29–59 years) participated in this study. Images were acquired using the 3.0-Tesla MR part of the Ingenuity TF hybrid positron emission tomography (PET)/MR system (Philips Healthcare, Cleveland, OH, USA). An in-house developed transaxial BB-FST2WI with SSTSE sequence was performed under a single breath-hold and with PPU gating. The variable refocusing flip-angle (VRFA) technique3 was employed for obtaining the black-blood effect. The sequence parameters were as follows: repetition time / equivalent echo time, 1 R-R interval / 77 ms; turbo spin echo factor, 77; fat suppression; spectral attenuated inversion recovery; section thickness, 7 mm; section gap, 0 mm; acquisition matrix, 244 × 157; in-plane reconstruction resolution, 0.74 × 0.75 mm2; parallel imaging acceleration factor, 2; number of signal averages, one; and scan duration; 10 R-R intervals. For PPU gating, the trigger point was set at the point showing the maximal upslope gradient in the peripheral pulse waveform. For each subject, two transaxial images of the upper/lower lung were obtained with 10 incremental trigger delay time points during a pulse cycle (Figure 2-3). Image analysis was performed using open-source software package ImageJ version 1.48 (National Institutes of Health, Bethesda, MD, USA). The assessment of signal suppression and contrast changes was made using the relative signal intensity ratio (RSIR) of the specific tissue to the muscle. A 1-cm2 circular reference region of interest (ROI) was marked on the erector spinae muscle. Each side of the lung field as well as the descending aorta, cardiac ventricles, pulmonary trunk, and mediastinal lymph node were manually contoured and extracted. The RSIR was defined as 100 × [(mean signal the area of interest) / (mean signal of the reference ROI); Figure 4)]. A relative intensity curve was generated by summing the values obtained from each volunteer and was plotted as a function of trigger delay time.Results
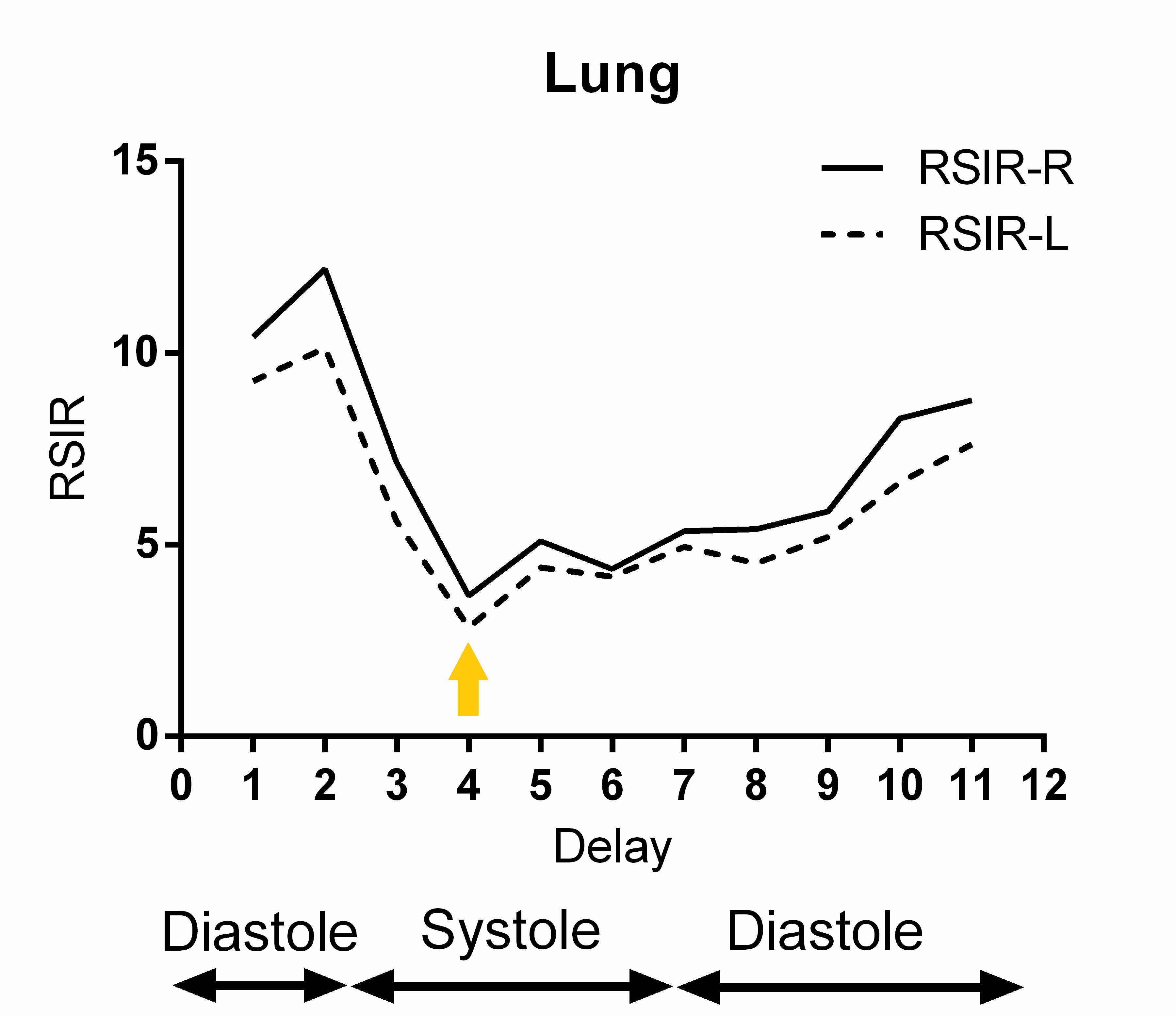
The average heart rate for the eight volunteers ranged from 58 to 72 bpm. Among the 10 serial images, pulmonary vascular signal was strongly suppressed on the images acquired within the mid-systolic phase of the cardiac cycle (as aforementioned in Figure 3). On the RSIR curve with trigger delay time, the mean RSIRs of the lung consistently decreased from 12.2 / 10.1 to 3.67 / 2.84 (right / left) with longer trigger delay time toward the mid-systole. The curve then gradually increased throughout the acquisition. The right and left correlation was excellent (Figure 5). Similar trends were observed for the aorta, ventricles, and pulmonary trunk. On the other hand, the mediastinal lymph node showed the highest RSIRs at the mid-systole. For each region, there were significant differences among the mean signals recorded in the four representative trigger delay time points, where the mid-systolic phase provided the strongest vascular suppression and the strongest lymph node contrast (p < 0.05 with repeated measures ANOVA and Tukey's test).Conclusions
The results of our study suggest that 2D-turbo spin-echo sequence with incremental trigger delay time is a feasible method for monitoring pulmonary vascular suppression during a whole cardiac cycle. The trigger delay time point corresponding to the mid-systolic phase is optimal for obtaining the maximum pulmonary vascular signal suppression, which could provide a high lesion conspicuity and good visibility of the lymph nodes on BB-FST2WI.Acknowledgements
This study has received funding by JSPS KAKENHI Grant Number JP16K19828.References
1. Kamei R, Watanabe Y, Sagiyama K, et al. Breath-hold lung MR imaging for nodule detection: Combination of 3D mDixon and black-blood fat-saturated HASTE sequences. RSNA 2015
2.Kamei R, Watanabe Y, Sagiyama K, et al. Breath-Hold Peripheral Pulse-Gated Black-Blood T2-Weighted Lung Magnetic Resonance Imaging with the Variable Refocusing Flip Angle Technique. ISMRM 2016
3. Yoneyama M, Nakamura M, Tabuchi T, Takemura A, Obara M. Optimization of 3D-variable refocusing flip angle RARE imaging for high-resolution volumetric black-blood angiography. Radiol Phys Technol 2012;5(2):270-276.
Figures