2148
Reproducibility and Methodological Considerations for Dissolved-Phase 129Xe Spectroscopy in Patients with Idiopathic Pulmonary Fibrosis.1Academic Unit of Radiology, University of Sheffield, Sheffield, United Kingdom, 2Academic Directorate of Respiratory Medicine, Sheffield Teaching Hospitals, Sheffield, United Kingdom, 3Infection, Immunity and Cardiovascular Disease, University of Sheffield, Sheffield, United Kingdom
Synopsis
The reproducibility of quantitative parameters of pulmonary gas-exchange function derived from 129Xe chemical shift saturation recovery (CSSR) and high-resolution spectroscopy (HRS) was evaluated in patients with idiopathic pulmonary fibrosis. Of the CSSR-derived parameters, surface-area-to-volume ratio was found to be most reproducible (intraclass correlation κ=0.756). Furthermore, the ratio of 129Xe signal in pulmonary red blood cells (RBC) to tissue/plasma (TP) from HRS exhibited good reproducibility (κ=0.760). The clinical interpretation of these results is discussed along with methodological considerations and their bearing on the future clinical potential of these techniques.
Purpose
The ratio of the spectral signals from inhaled hyperpolarized 129Xe dissolved in pulmonary red blood cells (RBC) to parenchymal tissue and plasma (TP) is a promising semi-quantitative measurement of pulmonary gas-exchange. 1 However, reproducibility of this method has not been assessed in patients with idiopathic pulmonary fibrosis (IPF).
Chemical shift saturation recovery (CSSR) is an alternative approach wherein NMR spectra are acquired at different delay times post-saturation of dissolved 129Xe signal, enabling estimation of lung microstructural parameters including alveolar septal thickness (ST) and surface-area-to-volume ratio (S/V). 2 Preliminary findings suggest that CSSR-derived ST is reproducible in healthy volunteers and patients with chronic obstructive pulmonary disease (COPD), 3 however the reproducibility of this method has yet to be evaluated in patients with IPF.
Methods
13 patients with IPF (70.3±5.2yrs, %-predicted DLCO (carbon monoxide diffusing capacity): 22.7-91.3%) underwent 129Xe spectroscopy at 1.5T. CSSR spectroscopy was implemented as previously reported, 3 and alveolar ST and S/V were estimated by fitting CSSR data with 1D diffusion models (Patz 2 and Chang 4). High-resolution spectroscopy (HRS) was also performed with: 1.8kHz bandwidth; 1024 spectral points; 90° flip angle; 1s TR, 10 acquisitions. The RBC/TP ratio was determined by fitting the mean complex spectrum as a sum of two Lorenztians, as previously described. 1
To assess short-term reproducibility, identical scanning protocols were performed twice on the same day. Reproducibility was quantified using intraclass correlation coefficient (ICC) between repeated scans. Correlations between 129Xe CSSR/HRS metrics and conventional pulmonary function tests were assessed using Spearman’s coefficient.
Results
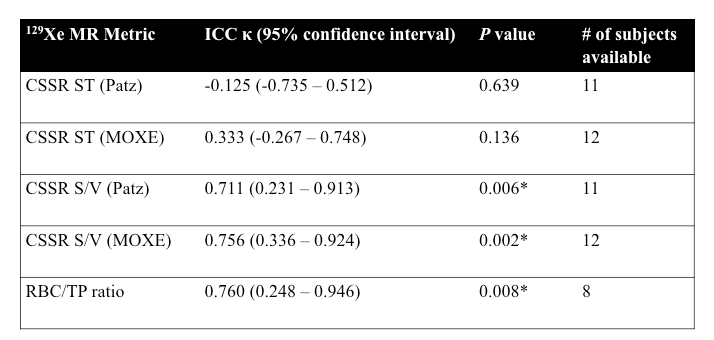
CSSR and HRS data were not acquired in one and three sessions, respectively. Furthermore, in two CSSR and three HRS datasets, SNR was insufficient for reliable analysis. The reproducibility of 129Xe spectroscopic metrics is summarized in Table 1.
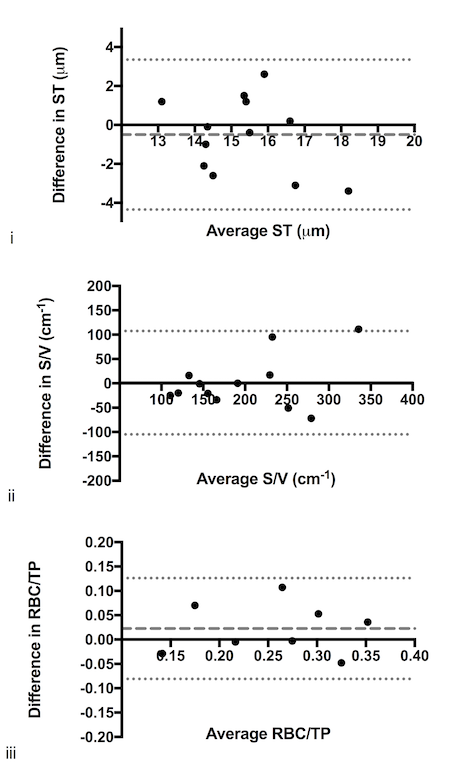
The CSSR-derived ST showed relatively poor reproducibility (ICC κ=0.333, P=0.136 for data analysed with MOXE), whilst the CSSR-derived S/V showed much better reproducibility (ICC κ=0.756, P=0.002). The RBC/TP ratio from HRS was also reproducible (ICC κ=0.760, P=0.008). Bland-Altman plots of the inter-scan variability of each parameter are shown in Figure 1.
The RBC/TP ratio correlated with carbon monoxide transfer coefficient, KCO (Spearman’s r=0.830, P=0.003), consistent with previous reports 1, although CSSR metrics did not.
Discussion
There are two principal points of discussion regarding the findings in this study: (i) clinical interpretation of the difference in reproducibility of 129Xe spectroscopy parameters; (ii) implementation of the RBC/TP method.
(i) The trend in reproducibility of CSSR-derived ST and S/V parameters in IPF patients is opposite to previous findings in COPD patients, 3 and raises questions as to whether current diffusion models of CSSR data 2,4 are applicable to IPF; i.e. the model of a uniform capillary septum with tissue sheath may be not be valid for heavily fibrosed tissue (where septal thickness may be heterogenous) associated with abnormal perfusion in addition to diffusion limitation.
In addition, the CSSR technique may be inherently more sensitive to variability in lung inflation level (and challenges with maintaining breath-hold) than the RBC/TP ratio technique in patients with IPF, however this postulation opposes a previous report that ST is less sensitive to inflation level than RBC/TP in healthy volunteers. 5 Regarding future clinical implementation, the RBC/TP method (single, averaged spectrum) is likely more robust to variations in SNR than CSSR (parametric model derived from several time-resolved spectra), and therefore may yield increased reproducibility.
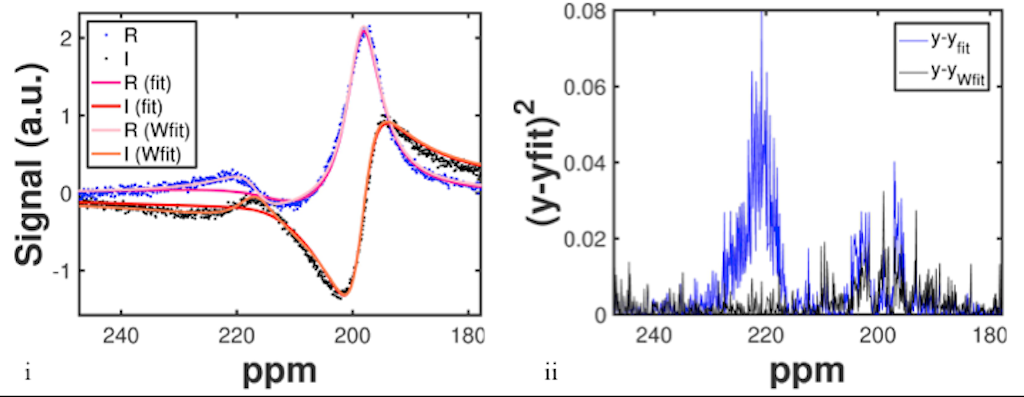
(ii) Despite preliminary evidence of good reproducibility of the RBC/TP ratio technique, in 6/13 patients, poor fits to the complex data were obtained at the first attempt. Statistically, fitting was more challenging in patients with severe disease; patients in which a good fit could not be achieved on the first attempt had significantly lower KCO than those whose data could be fitted successfully (Kolmogorov-Smirnov test, P=0.039). Data with poor initial fits were re-fitted by including the error function in the least-squares minimisation to apply additional weighting to the RBC peak (Wfit in Figure 2). This process yielded acceptable fits in all but two cases.
One recently proposed means to improve the complex fitting method is to consider the presence of a third dissolved-phase 129Xe peak, 6 however the associated additional fitting parameters increase the fitting algorithm’s complexity and requires considerable prior knowledge for reasonable initial guesses of fitting parameters.
Conclusion
The RBC/TP ratio derived from 129Xe spectroscopy was found to be more reproducible than the 129Xe CSSR-derived ST in IPF patients. Limitations of CSSR diffusion modelling in IPF, and methodological considerations for estimating the RBC/TP ratio, have been explored to assess clinical potential of these techniques in IPF patients.Acknowledgements
No acknowledgement found.References
1. Kaushik, S.S., Freeman, M.S., Yoon, S.W., et al., Measuring diffusion limitation with a perfusion-limited gas—Hyperpolarized (129)Xe gas-transfer spectroscopy in patients with idiopathic pulmonary fibrosis. Journal of Applied Physiology, 2014. 117(6):p.577-585.
2. Patz, S., Muradyan, I., Hrovat, M.I., et al., Diffusion of hyperpolarized 129 Xe in the lung: a simplified model of 129 Xe septal uptake and experimental results. New Journal of Physics, 2011. 13(1):p.015009.
3. Stewart, N.J., Horn, F.C., Norquay, G., et al., Reproducibility of quantitative indices of lung function and microstructure from (129) Xe chemical shift saturation recovery (CSSR) MR spectroscopy. Magnetic Resonance in Medicine, 2016. DOI: 10.1002/mrm.26310. [Epub ahead of print]
4. Chang, Y.V., MOXE: A model of gas exchange for hyperpolarized 129Xe magnetic resonance of the lung. Magnetic Resonance in Medicine, 2013. 69(3):p.884-890.
5. Qing, K., Mugler, J.P., Altes, T.A., et al., Assessment of lung function in asthma and COPD using hyperpolarized 129Xe chemical shift saturation recovery spectroscopy and dissolved-phase MRI. Nuclear Magnetic Resonance in Biomedicine, 2014. 27(12):p.1490-501.
6: Robertson, S.H., Virgincar, R.S., Bier, E.A., et al., Uncovering a third dissolved-phase 129Xe resonance in the human lung: Quantifying spectroscopic features in healthy subjects and patients with idiopathic pulmonary fibrosis. Magnetic Resonance in Medicine, 2016. DOI: 10.1002/mrm.26533. [Epub ahead of print]
Figures