2125
Perfusion Parameters at Dynamic Contrast-enhanced Breast MR Imaging are Associated with Disease-Specific Survival in Patients with Triple-Negative Breast Cancer1Radiology, Yonsei University College of Medicine, Seoul, Korea, Republic of
Synopsis
We investigated the association between perfusion parameters in pretreatment MR imaging and survival outcome. This retrospective study included 61 consecutive patients (median age, 50 years; range, 27-77 years) diagnosed with TNBC who underwent pretreatment DCE breast MR imaging and definitive surgery. The median follow-up time was 46.1 months. Among pretreatment variables, a higher ve value and higher peak enhancement at pretreatment MR imaging were significantly associated with worse disease-specific survival in patients with TNBC. With further validation, these perfusion parameters have the potential to aid in the pretreatment risk stratification of patients with TNBC and in evidence-based clinical decision support.
Purpose
To investigate the association between perfusion parameters in pretreatment MR imaging and survival outcome (disease-free survival [DFS], disease-specific survival [DSS]) in patients with triple negative breast cancer (TNBC).Methods
Sixty-one consecutive patients (median age, 50 years; range, 27-77 years) diagnosed with TNBC with or without axillary lymph node metastasis and who underwent pretreatment DCE breast MR imaging and definitive surgery were included. MR examinations were performed using one 3-T MR scanner (TrioTim; Siemens, Erlangen, Germany), of which T1-weighted dynamic contrast-enhanced MR imaging included one precontrast acquisition and six postcontrast bilateral axial acquisitions (TR/TE, 280/2.6; matrix, 512 × 343 pixels, field of view 340 × 340 mm; section thickness 3mm, no intersection gap). For calculation of perfusion parameters, post-processing of DCE MR data was performed with dedicated post-processing software (Olea Sphere v2.3, Olea Medical, La Ciotat, France). For model-based perfusion parameters, pharmacokinetic analysis of DCE-MRI data was performed based on the extended Tofts model. Values for signal enhancement ratio (SER) and peak enhancement were estimated directly from the time-signal intensity curves.
We retrospectively analyzed clinical-pathologic variables and MR imaging parameters. Cox proportional hazards models were used to analyze the hazard ratio (HR) with 95% confidence intervals (CI) for disease-free survival and disease-specific survival with variables obtainable before treatment and with post-treatment clinical-pathologic variables. Additionally, cutoff points were determined for perfusion parameters significant at univariate analysis using the Contal and O’Quigley method.
Results
The median follow-up time was 46.1 months (range, 13.9-58.4 months). Eleven of 61 (18.0%) patients had events and seven (11.4%) died from breast cancer. Among pretreatment variables, a larger tumor size on MR images (HR = 1.024, P = .003) was associated with worse DFS at univariate analysis. A higher Ktrans value was associated with worse DFS with borderline significance (HR = 1.113, P =.056). Among post-treatment variables, a larger pathologic tumor size at surgery (HR = 1.106, P < .001), presence of metastasis in surgically resected axillary LNs (HR = 9.382, P < .001), receipt of total mastectomy (HR = 10.205, P = .003) and not receiving radiation therapy (HR = 6.912, P = .001) were independently associated with worse DFS. At multivariate analysis of post-treatment variables, a larger pathologic tumor size at surgery (HR = 1.074, P = .005) and the presence of metastasis in surgically resected axillary LNs (HR = 5.789, P = .017) were associated with worse DFS.
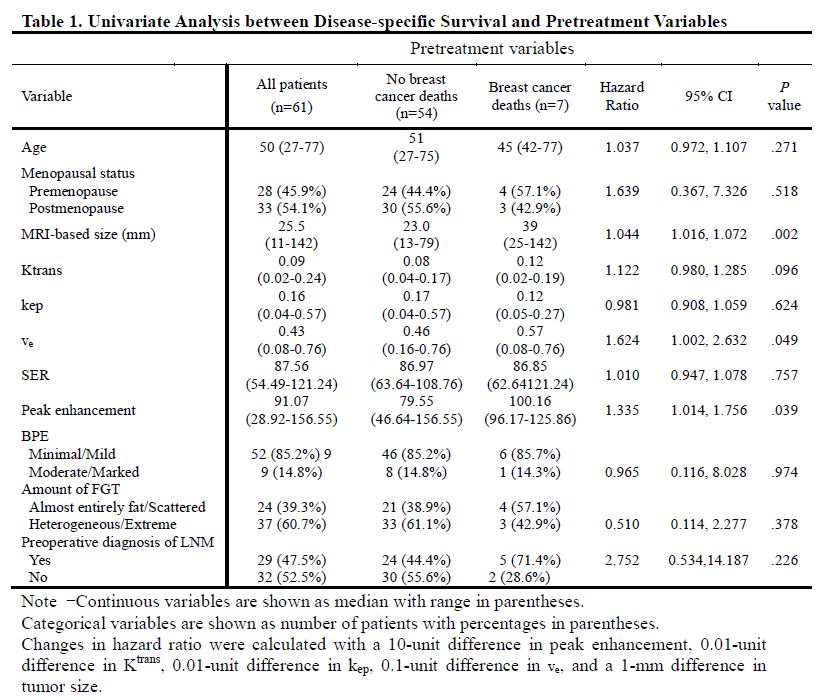
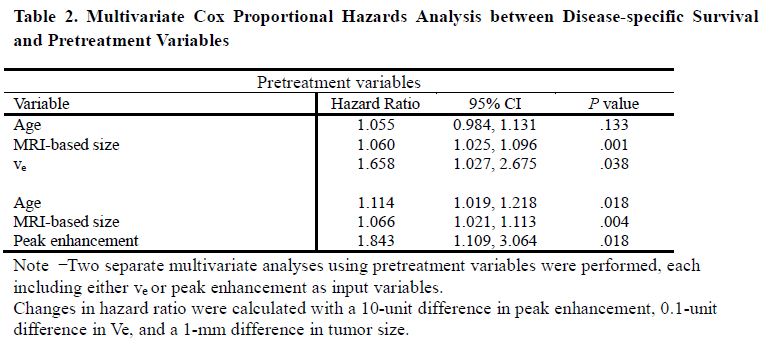
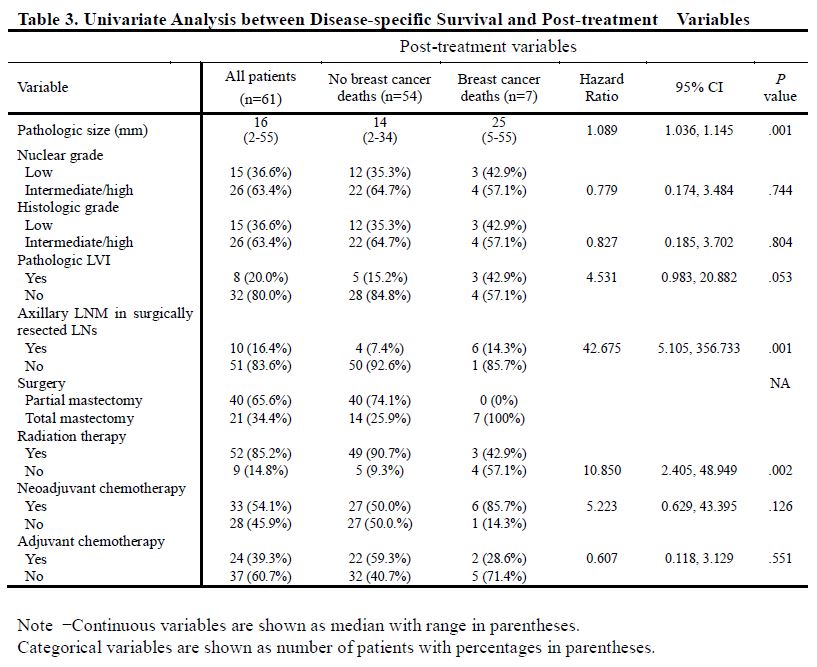
Among pretreatment variables, a higher ve value (HR = 1.624, P = .049), higher peak enhancement (HR = 1.335, P = .039), and a larger tumor size on pretreatment MR images (HR = 1.044, P = .002) were associated with worse DSS at univariate analysis. The statistically determined best cutoff points for perfusion parameters were as follows: 0.48 for ve and 96.17 for peak enhancement. A ve value greater than 0.48 (HR = 13.933, P = .014) and a peak enhancement value greater than 96.17 (HR = 13.933, P = .038) was associated with worse DSS. In multivariate pretreatment models for DSS, a higher ve value (HR=1.658, P=.038), higher peak enhancement (HR=1.843, P=.018) and a larger tumor size on MR images (HR=1.060, P=.001) were associated with worse DSS. In multivariate post-treatment models, a larger pathologic tumor size (HR=1.050 ,P=.042) and metastasis in surgically resected axillary lymph nodes (HR= 23.717 ,P =.002) were associated with worse DSS.
Conclusion
A higher ve value and higher peak enhancement at pretreatment MR imaging were significantly associated with worse disease-specific survival in patients with TNBC. After validation by large-scale studies, these perfusion parameters have the potential to aid in the pretreatment risk stratification of patients with TNBC and in evidence-based clinical decision support.Acknowledgements
We would like to thank Hye Sun Lee for her advice and assistance in statistical analysis.References
1. Moran MS. Should Triple-Negative Breast Cancer (TNBC) Subtype Affect Local-Regional Therapy Decision Making? Am Soc Clin Oncol Educ Book 2014; 34:e32-36
2. Dent R, Trudeau M, Pritchard KI, et al. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res 2007; 13:4429-4434
3. Kassam F, Enright K, Dent R, et al. Survival outcomes for patients with metastatic triple-negative breast cancer: implications for clinical practice and trial design. Clin Breast Cancer 2009; 9:29-33
4. Liu Y, Baglia M, Zheng Y, et al. ALDH1A1 mRNA expression in association with prognosis of triple-negative breast cancer. Oncotarget 2015; 6:41360-41369
5. Stirzaker C, Zotenko E, Song JZ, et al. Methylome sequencing in triple-negative breast cancer reveals distinct methylation clusters with prognostic value. Nat Commun 2015; 6:5899
6. Park VY, Kim EK, Kim MJ, Yoon JH, Moon HJ. Breast parenchymal signal enhancement ratio at preoperative magnetic resonance imaging: association with early recurrence in triple-negative breast cancer patients. Acta Radiol 2016; 57:802-808
7. Valero V. Carboplatin for early triple-negative breast cancer? Lancet Oncol 2014; 15:676-678
8. von Minckwitz G, Schneeweiss A, Loibl S, et al. Neoadjuvant carboplatin in patients with triple-negative and HER2-positive early breast cancer (GeparSixto; GBG 66): a randomised phase 2 trial. Lancet Oncol 2014; 15:747-756
9. de Kruijf EM, van Nes JG, van de Velde CJ, et al. Tumor-stroma ratio in the primary tumor is a prognostic factor in early breast cancer patients, especially in triple-negative carcinoma patients. Breast Cancer Res Treat 2011; 125:687-696
10. Dekker TJ, van de Velde CJ, van Pelt GW, et al. Prognostic significance of the tumor-stroma ratio: validation study in node-negative premenopausal breast cancer patients from the EORTC perioperative chemotherapy (POP) trial (10854). Breast Cancer Res Treat 2013; 139:371-379
11. Moorman AM, Vink R, Heijmans HJ, van der Palen J, Kouwenhoven EA. The prognostic value of tumour-stroma ratio in triple-negative breast cancer. Eur J Surg Oncol 2012; 38:307-313
12. Yim H, Kang DK, Jung YS, Jeon GS, Kim TH. Analysis of kinetic curve and model-based perfusion parameters on dynamic contrast enhanced MRI in breast cancer patients: Correlations with dominant stroma type. Magn Reson Imaging 2016; 34:60-65
13. Hammond ME, Hayes DF, Dowsett M, et al. American Society of Clinical Oncology/College Of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J Clin Oncol 2010; 28:2784-2795
14. Wolff AC, Hammond ME, Schwartz JN, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. J Clin Oncol 2007; 25:118-145
15. Kim MJ, Kim EK, Park S, Moon HJ, Kim SI, Park BW. Evaluation with 3.0-T MR imaging: predicting the pathological response of triple-negative breast cancer treated with anthracycline and taxane neoadjuvant chemotherapy. Acta Radiol 2015; 56:1069-1077
16. King V, Brooks JD, Bernstein JL, Reiner AS, Pike MC, Morris EA. Background parenchymal enhancement at breast MR imaging and breast cancer risk. Radiology 2011; 260:50-60
17. Tofts PS, Brix G, Buckley DL, et al. Estimating kinetic parameters from dynamic contrast-enhanced T(1)-weighted MRI of a diffusable tracer: standardized quantities and symbols. J Magn Reson Imaging 1999; 10:223-232
18. Grigoriu BD, Scherpereel A, Devos P, et al. Utility of osteopontin and serum mesothelin in malignant pleural mesothelioma diagnosis and prognosis assessment. Clin Cancer Res 2007; 13:2928-2935
19. Contal C, O'Quigley J. An application of changepoint methods in studying the effect of age on survival in breast cancer. Computational Statistics & Data Analysis 1999; 30:253-270
20. Kim JY, Kim SH, Kim YJ, et al. Enhancement parameters on dynamic contrast enhanced breast MRI: do they correlate with prognostic factors and subtypes of breast cancers? Magn Reson Imaging 2015; 33:72-80
21. Koo HR, Cho N, Song IC, et al. Correlation of perfusion parameters on dynamic contrast-enhanced MRI with prognostic factors and subtypes of breast cancers. J Magn Reson Imaging 2012; 36:145-151
22. Yi B, Kang DK, Yoon D, et al. Is there any correlation between model-based perfusion parameters and model-free parameters of time-signal intensity curve on dynamic contrast enhanced MRI in breast cancer patients? Eur Radiol 2014; 24:1089-1096
23. Gujam FJ, Edwards J, Mohammed ZM, Going JJ, McMillan DC. The relationship between the tumour stroma percentage, clinicopathological characteristics and outcome in patients with operable ductal breast cancer. Br J Cancer 2014; 111:157-165
24. Gillies RJ, Kinahan PE, Hricak H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2015:151169
25. Lee JA, Kim KI, Bae JW, Jung YH, An H, Lee ES. Triple negative breast cancer in Korea-distinct biology with different impact of prognostic factors on survival. Breast Cancer Res Treat 2010; 123:177-187
26. Mamounas EP, Anderson SJ, Dignam JJ, et al. Predictors of locoregional recurrence after neoadjuvant chemotherapy: results from combined analysis of National Surgical Adjuvant Breast and Bowel Project B-18 and B-27. J Clin Oncol 2012; 30:3960-3966
27. Pickles MD, Lowry M, Gibbs P. Pretreatment Prognostic Value of Dynamic Contrast-Enhanced Magnetic Resonance Imaging Vascular, Texture, Shape, and Size Parameters Compared With Traditional Survival Indicators Obtained From Locally Advanced Breast Cancer Patients. Invest Radiol 2016; 51:177-185
28. Nguyen PL, Taghian AG, Katz MS, et al. Breast cancer subtype approximated by estrogen receptor, progesterone receptor, and HER-2 is associated with local and distant recurrence after breast-conserving therapy. J Clin Oncol 2008; 26:2373-2378
29. Jena A, Mehta SB, Taneja S. Optimizing MRI scan time in the computation of pharmacokinetic parameters (K(trans) ) in breast cancer diagnosis. J Magn Reson Imaging 2013; 38:573-579
30. de Bazelaire C, Calmon R, Thomassin I, et al. Accuracy of perfusion MRI with high spatial but low temporal resolution to assess invasive breast cancer response to neoadjuvant chemotherapy: a retrospective study. BMC Cancer 2011; 11:361
31. Li KL, Henry RG, Wilmes LJ, et al. Kinetic assessment of breast tumors using high spatial resolution signal enhancement ratio (SER) imaging. Magn Reson Med 2007; 58:572-581
32. Li KL, Wilmes LJ, Henry RG, et al. Heterogeneity in the angiogenic response of a BT474 human breast cancer to a novel vascular endothelial growth factor-receptor tyrosine kinase inhibitor: assessment by voxel analysis of dynamic contrast-enhanced MRI. J Magn Reson Imaging 2005; 22:511-519
33. Kuroi K, Toi M, Ohno S, et al. Comparison of different definitions of pathologic complete response in operable breast cancer: a pooled analysis of three
Figures