2118
Comparison of whole tumor and single slice ROIs for measuring ADC in breast cancer1University of California, San Francisco, CA, United States
Synopsis
Diffusion weighted imaging is a promising technique to monitor treatment response in patients undergoing pre-surgical chemotherapy, but manually drawn whole tumor measurements are time-consuming and subject to inter-user variability. In this study of 60 patients with sequential DWI exams during treatment, we measured apparent diffusion coefficient (ADC) from whole tumor ROIs and from a single central slice of the tumor. We found strong agreement in ADC between the two methods, suggesting that a slice from the center of the tumor may accurately represent the ADC of the entire tumor.
Background
Breast MRI is increasingly used to assess response to neoadjuvant (pre-surgical) chemotherapy. While dynamic contrast enhanced (DCE) MRI provides detailed information about anatomy and enhancement kinetics, diffusion weighted imaging (DWI) shows alterations in the tumor microenvironment before changes in tumor size [1] and vasculature are measurable. Methods vary for delineating tumor regions of interest (ROI) on DWI and determining tumor apparent diffusion coefficient (ADC). While manually drawn whole tumor ROIs, drawn on all slices in which the tumor is visible, allow for precise delineation of the tumor and more complete ADC measurement, this technique is time consuming and is subject to reader variability. This study compared the agreement between ADC from manually drawn whole tumor ROIs and ADC from a representative ROI drawn on a single-slice in the center region of the tumor.Methods
Sixty patients undergoing neoadjuvant chemotherapy for locally advanced breast cancer had sequential MRIs to monitor treatment response as part of an ongoing institutional review board-approved, HIPAA compliant clinical trial. All patients gave informed consent. ADC was measured on a total of 98 exams. DWI was acquired at 1.5T (n=43) or 3T (n=17) using a 2D DW SE-EPI sequence and a dedicated breast coil. Active fat suppression was used, and bilateral axial DWI images were acquired prior to the administration of the contrast for DCE imaging. Two or more b-values, b=0 and b=800 mm2/sec, were used for DWI acquisitions.
ADC maps were generated using in-house software, and whole tumor ROIs were delineated by one of two readers (JG and MR). Tumor was identified using post-contrast DCE subtraction images based on high signal intensity. Tumor was then localized on the ADC map using similar breast anatomical structures and corresponding low signal intensity on the ADC map and high signal intensity at high b-value (b600 or b800). Tumor was manually delineated on the ADC map, excluding surrounding fat and tissue to eliminate partial volume effects. Tumor necrosis, clip artifacts, and areas exhibiting T2 shine-through were also excluded. ROIs were drawn on contiguous slices to include all suspected tumor. A representative single slice was then selected in the center of the tumor.
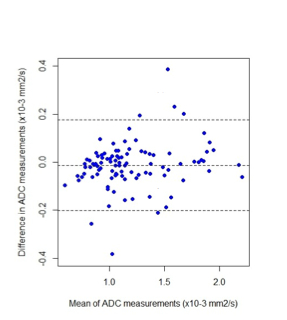
Mean ADCs from the whole tumor and single-slice ROIs were compared using a Bland-Altman plot. Impact of tumor size and tumor morphology on the difference of ADC measurements was assessed using a linear mixed-effects model.
Results
Preliminary results show a strong positive correlation between whole tumor and single-slice measurements of ADC (r=0.9644, p<0.05). The Bland-Altman plot shows no significant systematic difference between single-slice and whole tumor ADC measurements. The line of equality (mean difference = 0) is within the confidence interval (CI) of the mean difference (-0.014 × 10-3 mm2/s, 95% CI (-0.033, 0.0058 × 10-3 mm2/s)). The difference between single-slice and whole tumor ROI ADC measurements lies within the lower and upper limits of agreement for more than 90% of cases (-0.20 to 0.18 × 10-3 mm2/s). Mixed-effects modeling showed no evidence of an effect on difference in the two methods by tumor volume or tumor morphology. Reader variability is currently being assessed.Conclusion
Single-slice measures of breast tumor ADC show strong agreement with whole tumor measures of ADC, indicating that the single-slice method may be an accurate representation of whole tumor ADC. Continuing studies will test the relative predictive performance of whole tumor and single-slice ADC for predicting response to treatment.Acknowledgements
No acknowledgement found.References
1. Pickles MD, Magn Reson Imaging, 2006 Sep;24(7):843-7.Figures