2108
3D Volumetric Noncompressive Breast MR Elastography1Radiology, Mayo Clinic, Rochester, MN, United States, 2Radiology, Mayo Clinic, Scottsdale, AZ, United States
Synopsis
Sternum drivers for breast MRE can produce shear waves in breasts without breast compression effect, which can result in increased breast stiffness due to tissue nonlinearity. A recent 5-slice 2D GREMRE sequence study found sternum driver MRE was a very reproducible method. In our current study, we were able to use 40-slice 3D GREMRE volumetric MRE sequence to compute volumetric breast elastograms in patients.
Introduction
In vivo breast cancer patient studies have shown that tumor mechanical property - measured by MR-based elastography (MRE) [1] or ultrasound-based elastography[2, 3] - is a potentially highly specific biomarker in differentiating benign lesions from malignancies. Therefore, there is a good opportunity for MRE to advance the specificity of breast MRI by offering additional information of breast mechanical properties [1, 4-6].
We originally designed sternum drivers for breast MRE to avoid breast compression effect in 2011. A recent study used sternum breast MRE driver found this method is very reproducible at a 3T MRI system [7]; however, there were only five 2D GREMRE slices collected in the breasts, which raises questions of the accuracy.
Therefore, in our current study, we used true 3D GREMRE volumetric sequence to collect 40 axial slices at 3 polarization directions to compute 3D volumetric breast elastograms at 3T. We hypothesize that it is feasible to measure breast tissue stiffness using the 3D volumetric noncompressive breast MRE technique.
Methods
Subjects: This prospective and HIPAA compliant study was IRB approved. Female volunteers who did not have known breast diseases were recruited in the study after they signed the written consent forms. In total, 5 female volunteers underwent breast MRE on an MR750w 3T scanner (GE, Wisconsin, USA), and the other 5 on an HDxt 3T scanner (GE, Wisconsin, USA). In the total of 10 volunteers, age = 36.9 (28.8, 45.0) years, weight = 70.7 (61.5, 79.8) kg, height = 1.64 (1.59, 1.69) m, body mass index (BMI) = 26.3 (22.5, 30.1) kg/m2.
Breast MRE: 3D breast MRE[8] was optimized for 3T with a smaller flip angle (8 degree). For both scanners (MR750w 3T and HDxt 3T), their standard breast RF coils were used. A noncompressive MRE breast driver (2 x 0.6 x 22, cm) was positioned between the coil and the volunteers’ sternum (prone position) during the MRI/MRE exams[6]. 3D-GREMRE was used with the following major parameters[9]: vibration frequency = 40 Hz; FOVx/y/z = 38/38/14.4 cm; flip angle = 8°; TR = 22.2 – 22.9 ms, TE = 15.9 - 18.1 ms (fat/water in-phase); axial bilateral imaging plane; matrix = 96 (72) × 96 (72) × 40; 8 motion cycles per 9 TRs (3 phase offsets); motion sensitivity (MENC) = 12.3 micron/radian; motion encoding directions = x/y/z; scan time = 5’25’’ - 5’42” (free breathing). 3D wave images were processed with 3D multi-model direct inversions without any need of directional filtering[10], generating 3D elastograms of bilateral breasts. High quality T1-weighted or T2-weighted anatomic breast MR images were used to identify breast tissue and 12 big ROIs was drawn to include the majority of breast tissue (fat and fibroglandular tissue) in the middle 12 slices of elastograms, excluding low SNR areas. Global mean breast tissue stiffness values were measured and averaged in the 12 ROIs for the left and right breasts in the 10 volunteers.
Statistical Analysis: The averaged global breast stiffness, as well as age, weight, height and BMI were compared between volunteers who underwent the two MRI systems (MR750w vs. HDxt). P values were calculated using one-way ANOVA (analysis of variance), with a value of less than 0.05 indicating a statistically significant difference. JMP Pro 11 (SAS, Cary, NC, USA) was used for analysis.
Results and Discussions
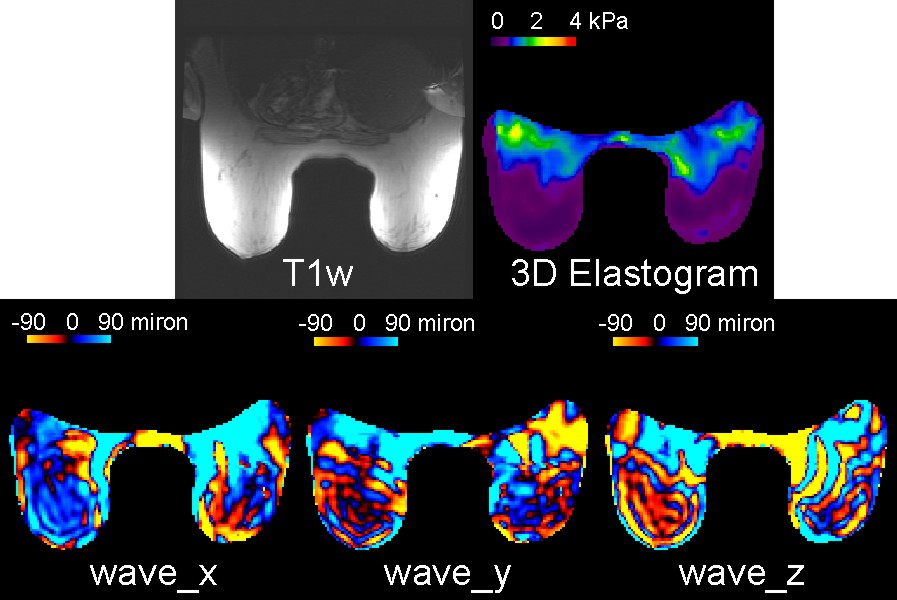
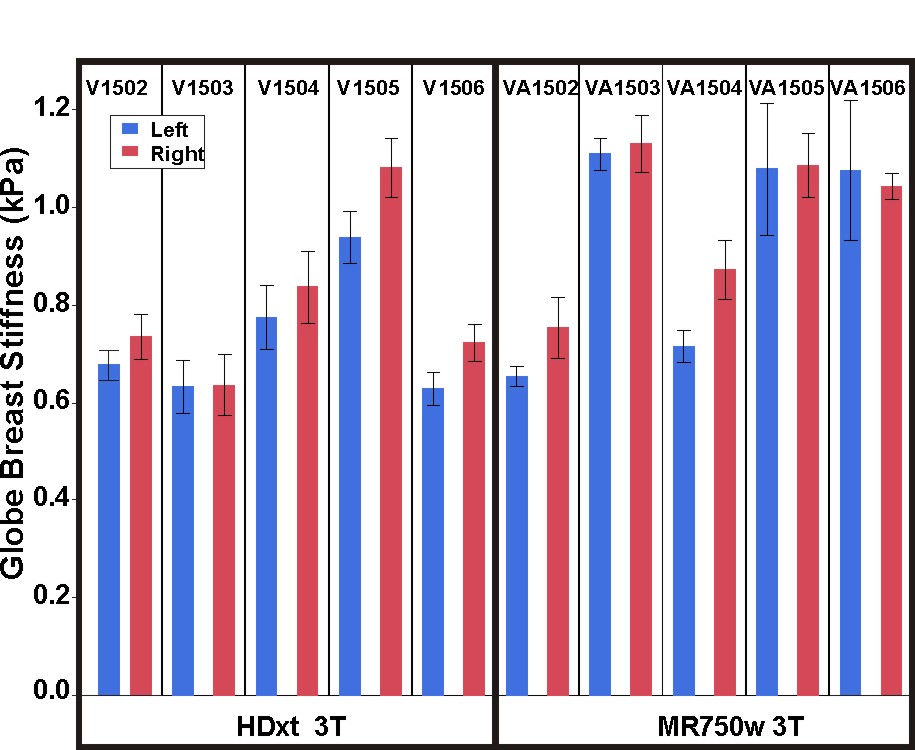
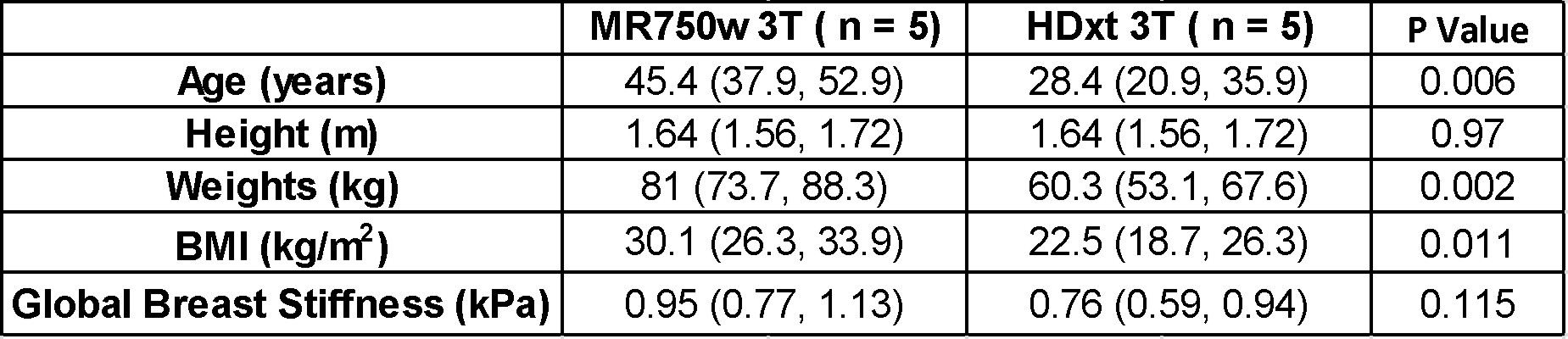
Figure 1 shows the example MRE images of one volunteer. Although attenuated by the fat tissue, shear waves generated from the chest wall (inside the breasts) and skin propagated to the middle of the two breasts. Note in the posterior part the two breasts, the local breast stiffness values were elevated. This was caused by the compression effect [11] when the breasts were compressed by the patient support pad. The patient pad needs an optimization so that it will not contact and compress the breast tissue. Figure 2 shows the left and right global breast stiffness for each volunteer, grouped by the 3T systems that they underwent. The volunteers who underwent MR750w were 17 years older (p = 0.006) than these who underwent HDxt 3T system; the two volunteer groups did not have a statistically significant difference in global breast stiffness: 0.95 (0.77, 1.13) kPa vs. 0.76 (0.59, 0.94) kPa, p = 0.115 (Figure 3). However, the lack of significance could be due to the small volunteer number.Conclusions
3D volumetric noncompressive breast MRE successfully provided breast tissue stiffness measurements at two different 3T systems. Our next step is to recruit more breast cancer patients to evaluate the clinic utility of improving the specificity of breast MRI.Acknowledgements
No acknowledgement found.References
No reference found.Figures