2106
Detection and Morphology of Breast Lesions with Very Early Phase of Ultrafast Dynamic Contrast Enhanced MRI using Compressed Sensing Reconstruction1Diagnostic Imaging and Nuclear Medicine, Kyoto University Graduate School of Medicine, Kyoto, Japan, 2Kyoto University Graduate School of Medicine, Kyoto, Japan, 3Division of Clinical Radiology Service, Kyoto University Hospital, Kyoto, Japan, 4MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany, 5Breast Surgery, Kyoto University, Kyoto, Japan
Synopsis
Using ultrafast DCE MRI (UF-DCE)with compressed sensing reconstruction, detection rate and morphology of breast lesions on very early phase images within 1 minutes post contrast injection were compared to those on full diagnostic protocol (FDP). Almost all (95%) of the lesions reported on FDP were identified on UF-DCE. Size of the lesions were slightly smaller on UF-DCE but within-2mm difference in 96% of masses. Considering that wash-in kinetic information can be obtained by UF-DCE, the current data of equivalent lesion detection, size and morphology evaluation on UF-DCE support its application to abbreviated breast MRI protocol.
INTRODUCTION
The breast dynamic contrast enhanced magnetic resonance imaging (DCE-MRI) is regarded as the most sensitive method for detecting breast lesions, although standard full diagnostic protocol (FDP) to evaluate both kinetic and morphological information normally takes 25 minutes. Some advocated the use of an abbreviated protocols consisting of pre and one post contrast images with reduced scanning time while maintaining high sensitivity [1-7]. Thanks to the recent technical advancement, ultrafast DCE (UF-DCE) acquisition becomes possible using time-resolve angiography with stochastic trajectories (TWIST) sequence [8], or 3D volumetric interpolated breath-hold examination (VIBE) sequence with compressed sensing reconstruction. The latter new protocol allows us to obtain images with less than 4 seconds time frame and 1 mm in-plane resolution, which enables wash-in kinetics, detect small lesions and capture detailed morphology as in FDP. The purpose of this analysis focused on 1) detection of enhanced lesions and 2) lesion size and morphology assessment of UF-DCE with standard FDP as reference images.METHODS
Study population consists of 28 consecutive patients who underwent Breast MRI with UF-DCE protocol to evaluate suspected or known breast cancers from April to August 2016 with histopathological diagnosis of the main lesions.
MR scan was performed using a 3-T system (Skyra; Siemens AG) equipped with a dedicated 16-channel breast array coil. Breast MRI studies were performed with a 3.0T scanner (MAGNETOM Trio, A Tim System, Siemens AG) with 18-channel dedicated bilateral breast coil. As a part of standard MRI (i.e. full diagnostic protocol:FDP) T2-weighted, T1-weighted, Diffusion weighted and fat-suppressed T1-wighted DCE images were obtained. Fat-suppressed T1-weighted DCE images; pre-contrast and two post-contrast, two times at 1–2 and 5–6 min after gadolinium injection, whole breast axial scanning in high temporal resolution for 1min (3D-VIBE: TR/TE 3.70/1.36ms, FA 15 and FOV 330 mm×330 mm, matrix 384x269, thickness 1.0 mm), post contrast at 2–5 min after gadolinium injection whole breast coronal scanning in high spatial resolution (3D-VIBE: TR/TE 4.01/1.63ms, FA 15, FOV 330 mm×330 mm, matrix 512x461, thickness 0.8mm). Infused gadolinium contrast materials were gadobutrol (Gadovist, Bayer. Germany) at a dose of 0.1 ml/kg power injected at a speed of 2.0 ml/s and flushed with 20 ml at a speed of 2.0 ml/s of saline at the same rate.
UF-DCE acquisitions were obtained at a very early phase; 15 seconds before injection and 1 min after gadolinium injection (TR/TE 5.0/2.5, FA 15, FOV 360 mm×360 mm, matrix 384x269, thickness 2.5 mm ,CS acceleration=16.5, temporal resolution 3.7 sec for 20 time flames). CS reconstruction was conducted with number of iterations of 30, which is determined as the optimal value in our test series.
Image evaluation: 1) Detection rate of enhanced lesions was calculated. Lesions reported as Category 3 or above for standard FDP were used as a reference. On UF-DCE, all 20 images and minimal intensity projection (MIP) images were reviewed to identify enhancing lesions. 2) For identified lesions, its size (maximum diameter) and morphology ( mass and non-mass enhancement: NME) were evaluated based on BI-RADS MRI 2013. The data were compared to those in reports based on FDP. Lesion size between UF-DCE and FDP was compared using Wilcoxon’s signed rank test.
RESULTS
In total 44 enhancing lesions (28 main and 16 secondary/associated lesions) were identified. Among them, 42 (95%) lesions were detected by UF-DCE. Size and detailed morphological assessment was performed for 39 lesions (26 masses and 13 NME).
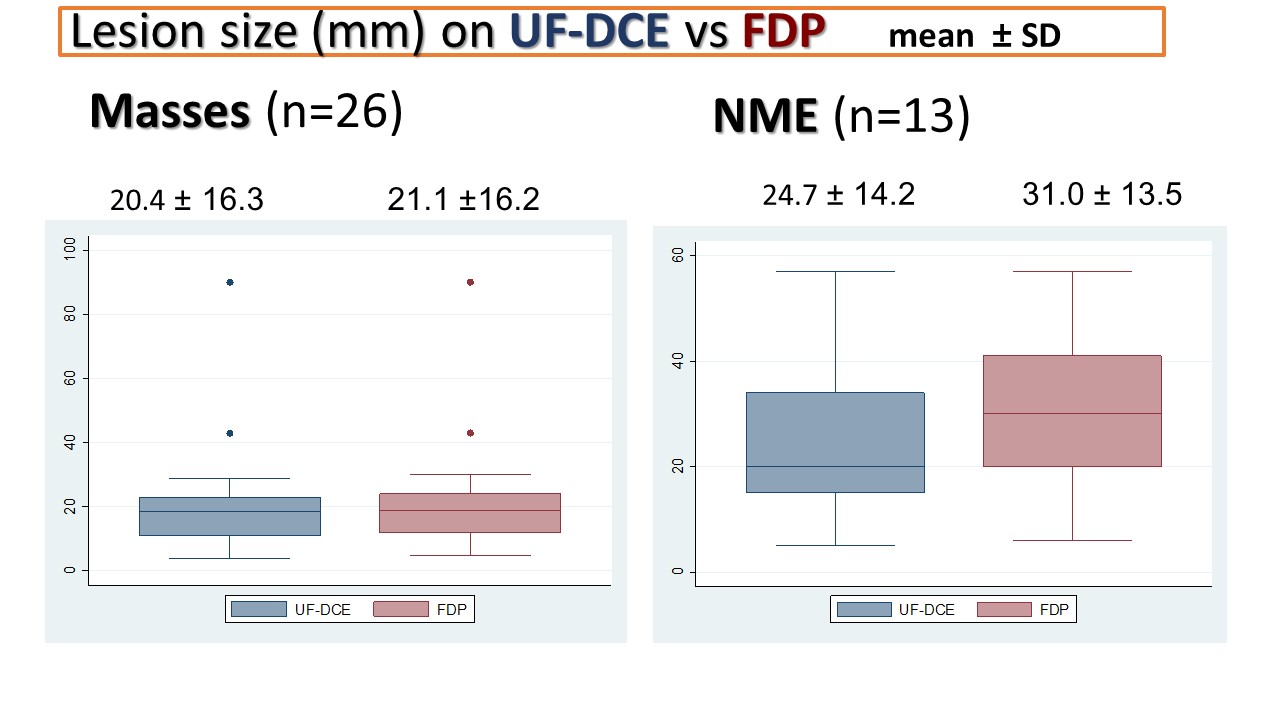
Size of the mass was slightly smaller on UF-DCE but within 2mm difference in 25 lesions 96%. NME tended to be measured smaller on UF-DCE (mean 24.7mm) compared with FDP (31.0 mm, p=0.005).
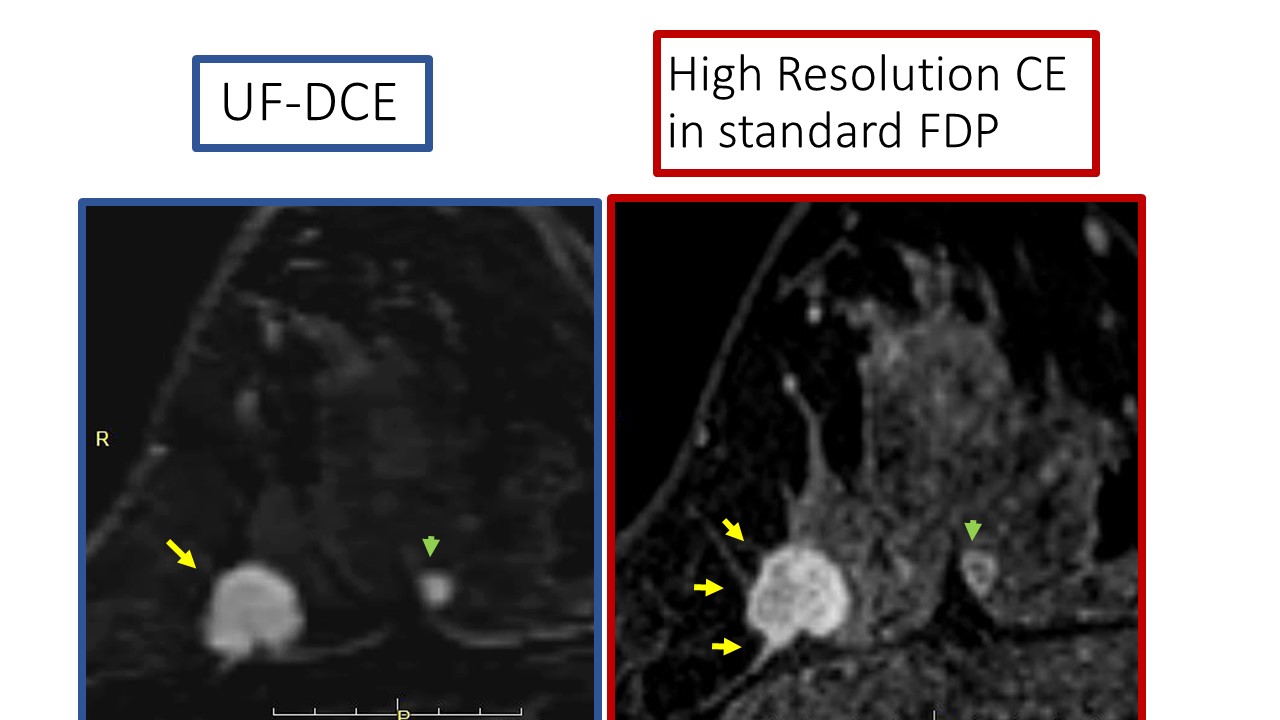
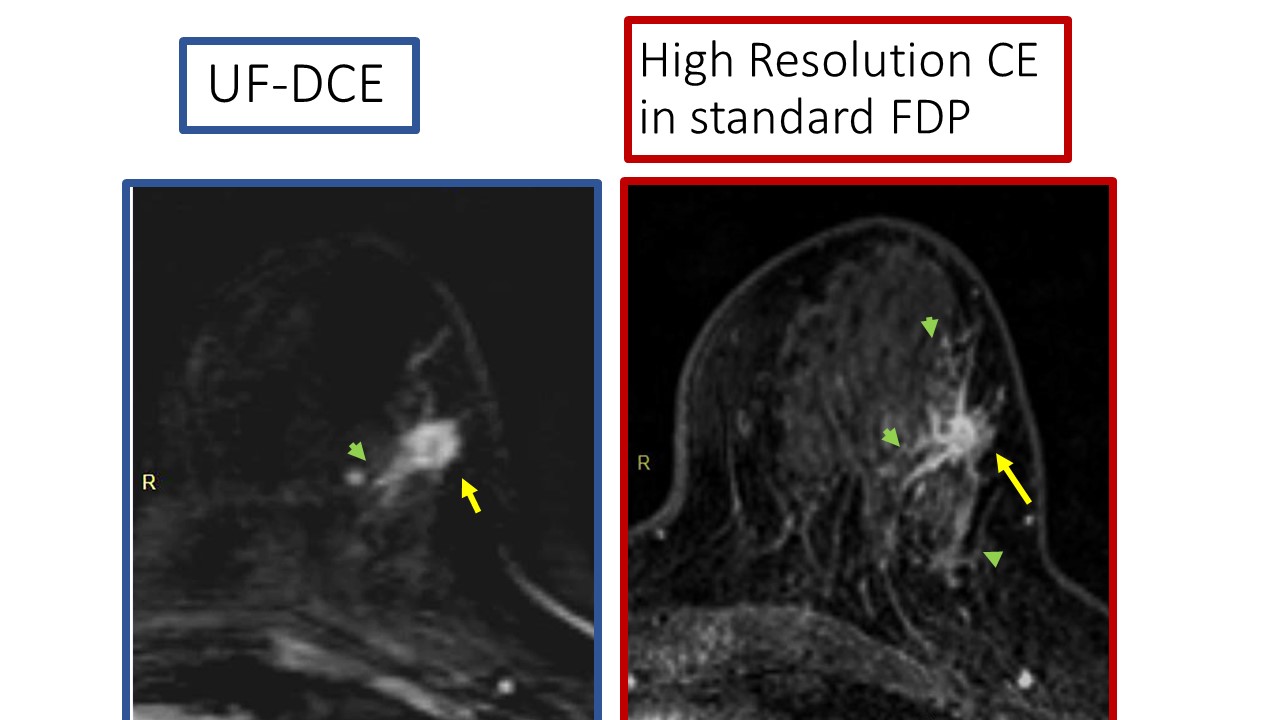
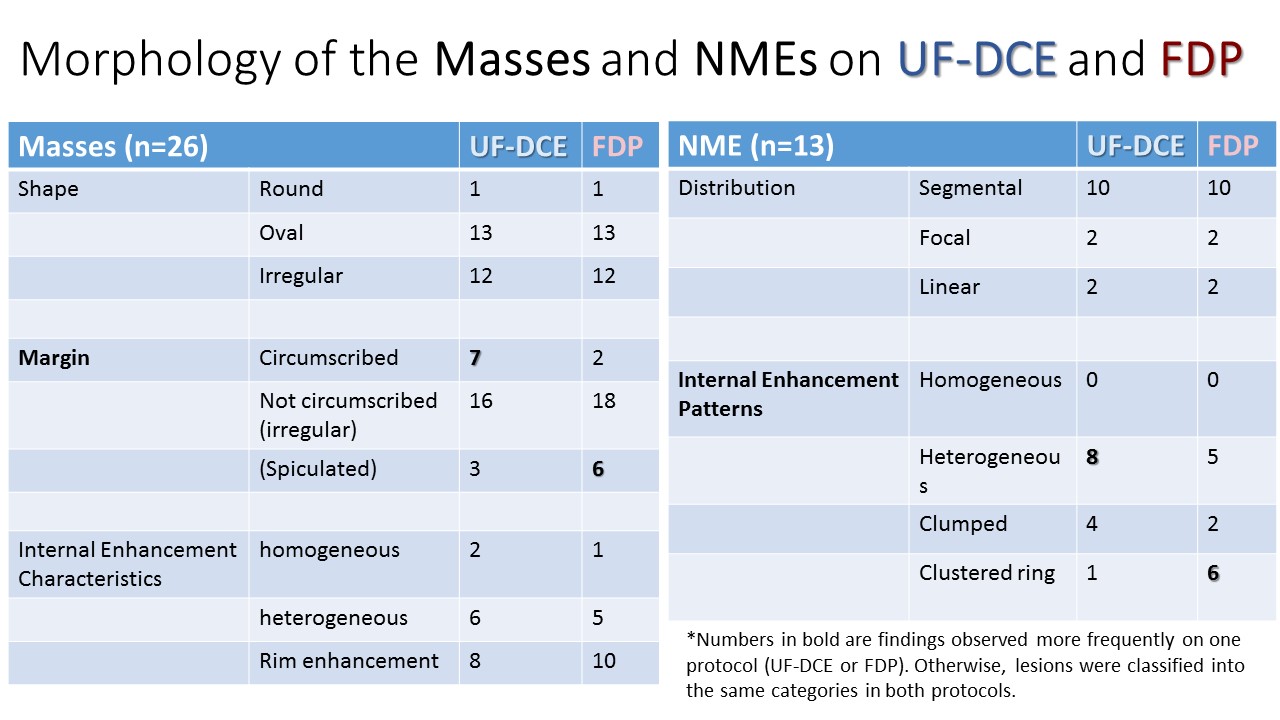
In morphology, shape of the mass and distribution of the NME completely agreed between UF-DCE and DFP. Margin of the mass disagree on 5 out of 26 lesions. In particular, 5 masses were classified as circumscribed on UF-DCE while irregular on FDP. Clustered ring were difficult to identify on UF-DCE and found positive in only 1 one 6 NME which were classified as positive on DFP. Two representative cases are shown in figures. These results were summarized in graph (figure 3) and a table and
DISCUSSIONS AND CONCLUSIONS
Most of the lesions reported on FDP were identified on UF-DCE. Massess were slightly smaller on UF-DCE but within-2mm difference and were fairly accurate. There was a discrepancy in size and presence of clustered ring on NME. Considering that wash-in kinetic information can be obtained by UF-DCE within one minutes, the current data demonstrating FDP-equivalent lesion detection and mass size on UF-DCE support potential application to a new abbreviated breast MRI with detailed morphology information.Acknowledgements
We thank Dr.Katsutoshi Murata and Yuta Urushibata, Siemens Japan, for their technical support in this work. This work was partly supported by Grant-in-Aid for Scientific Research on Innovative Areas “Initiative for High-Dimensional Data-Driven Science through Deepening of Sparse Modeling”, and Grant-in-Aid for Scientific Research (C) “Evaluation of Wash in Phase using Ultrafast MRI of the Breast.References
1: Kuhl CK, et al. Abbreviated breast magnetic resonance imaging (MRI): first postcontrast subtracted images and maximum-intensity projection-a novel approach to breast cancer screening with MRI. J Clin Oncol. 2014 Aug 1;32(22):2304-10.
2: Mango VL, et al. Abbreviated protocol for breast MRI: are multiple sequences needed for cancer detection? Eur J Radiol. 2015 Jan;84(1):65-70.
3: Grimm LJ, Soo MS, Yoon S, Kim C, Ghate SV, Johnson KS. Abbreviated screening protocol for breast MRI: a feasibility study. Acad Radiol. 2015 2(9):1157-62.
4: Heacock L, et al. Evaluation of a known breast cancer using an abbreviated breast MRI protocol: Correlation of imaging characteristics and pathology with lesion detection and conspicuity. Eur J Radiol. 2016 (4):815-23.
5: Machida Y, et al. Feasibility and potential limitations of abbreviated breast MRI: an observer study using an enriched cohort. Breast Cancer. 2016 Aug 2. Aug 2. [Epub ahead of print]
6: Moschetta M, et al. Abbreviated Combined MR Protocol: A New Faster Strategy for Characterizing Breast Lesions. Clin Breast Cancer. 2016 (3):207-11.
7: Jain M, at al. FAST MRI breast screening revisited. J Med Imaging Radiat Oncol. 2016 Jul 27. doi: 10.1111/1754-9485.12502. [Epub ahead of print]
8: Mann RM et al. A novel approach to contrast-enhanced breast magnetic resonance imaging for screening: high-resolution ultrafast dynamic imaging. Invest Radiol 2014; 49:579-585
Figures